
Airplane ear
Conditions
Overview
Airplane ear is stress on the eardrum that happens when the air pressure in the middle ear and the air pressure outside the ear are out of balance. Airplane ear might happen on an airplane that's climbing after takeoff or going lower for a landing.
Airplane ear also is called ear barotrauma, barotitis media and aerotitis media.
Self-care steps, such as yawning, swallowing or chewing gum, usually can improve airplane ear symptoms. But a severe case of airplane ear might need medical help.
Symptoms
Airplane ear can happen in one or both ears. Common symptoms of airplane ear include:
- Discomfort in the ear.
- Feeling of fullness or stuffiness in the ear.
- Muffled hearing or some hearing loss.
Symptoms of severe airplane ear might include:
- Severe pain.
- Increased pressure in the ear.
- Worse hearing loss.
- Ringing in the ear, called tinnitus.
- Feeling of spinning, called vertigo.
- Bleeding from the ear.
When to see a doctor
For ear discomfort or fullness or muffled hearing that lasts more than a few days, or for severe symptoms, make a medical appointment.
Causes
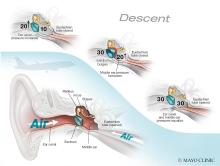
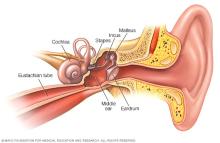
Airplane ear happens when the air pressure in the middle ear and the air pressure inside the airplane don't match. The mismatch keeps the eardrum, also called the tympanic membrane, from moving as usual.
A narrow passage called the eustachian tube connects the middle ear to the back of the nose and throat. The eustachian tube keeps air pressure even.
When an airplane climbs or goes lower, the air pressure changes fast. The eustachian tube often can't react fast enough. That causes the symptoms of airplane ear.
Swallowing or yawning opens the eustachian tube. The opening lets the middle ear get more air. This equals out the air pressure.
Airplane ear also can be caused by:
- Scuba diving.
- Hyperbaric oxygen chambers.
Riding an elevator in a tall building or driving in the mountains also can cause a minor bout of airplane ear.
Risk factors
Anything that blocks the eustachian tube or keeps it from working as usual can increase the risk of airplane ear. Common risk factors include:
- A small eustachian tube, especially in infants and toddlers.
- Common cold.
- Sinus infection.
- Hay fever, also called allergic rhinitis.
- Middle ear infection, also called otitis media.
- Sleeping on an airplane while it's going up or down. This prevents yawning or swallowing or doing anything to equal out the pressure in the ears.
Complications
Airplane ear usually isn't serious and gets better with self-care. Rarely, complications can happen when the condition is serious or long-lasting. Also, complications can happen if there's damage to the middle or inner ear.
Rare complications may include:
- Hearing loss that can't be restored.
- Ongoing ringing in the ears, called chronic tinnitus.
- Ongoing dizziness, called vertigo.
Prevention

To prevent or avoid airplane ear, follow these tips:
- Yawn and swallow during takeoff and landing. These moves open the eustachian tubes. Sucking on candy or chewing gum can make swallowing easier.
- Use the Valsalva maneuver during takeoff and landing. Gently blow, as if blowing the nose, while pinching the nostrils. Keep the mouth closed. Repeat several times, especially while landing. This can keep the pressure between the ears and the airplane cabin equal.
- Don't sleep during takeoffs and landings. Stay awake to do the self-care moves to keep pressure in the ears equal.
- Change travel plans. If possible, don't fly with a cold, a sinus infection, a stuffy nose or an ear infection. If you've had recent ear surgery, talk to your healthcare professional about when it's safe to travel.
- Use a nasal spray. For a stuffy nose, use a nasal spray about 30 minutes to an hour before takeoff and landing. Don't use too often or for too long. Nasal sprays taken over 3 to 4 days can make stuffiness worse.
- Use decongestant pills with care. Decongestants taken by mouth might help if taken 30 minutes to an hour before an airplane flight. Don't take decongestants if you have heart disease, a heart rhythm disorder or high blood pressure or if you're pregnant.
- Take allergy medicines. People with allergies can take their medicine about an hour before the flight.
- Try filtered earplugs. These earplugs keep the pressure equal during takeoffs and landings. Get them at drugstores, airport gift shops or hearing clinics. But you'll still need to yawn and swallow to relieve pressure.
A healthcare professional may place tubes or a balloon in the eardrum to keep the eustachian tube open to help people who get severe airplane ear and must fly often. It also can help people having hyperbaric oxygen therapy to heal wounds. The tubes help fluid drain, keep the middle ear open, and keep the pressure between the outer ear and middle ear equal.
Helping children prevent airplane ear
To help young children:
- Get them to swallow. Give babies or toddlers a bottle to suck on during takeoffs and landings to keep them swallowing. A pacifier also might help. Have children sit up while drinking. Children older than 4 can chew gum or drink or blow bubbles through a straw.
- Don't use decongestants. Decongestants aren't recommended for young children.
Diagnosis
Diagnosis of airplane ear, also called ear barotrauma, is based on medical history and an exam of the ear with a lighted tool called an otoscope.
Treatment
For most people, airplane ear heals with time. When the symptoms don't go away, treatments to even out the pressure might help symptoms of airplane ear.
Medicines
These medicines might help symptoms of airplane ear:
- Decongestant nasal sprays.
- Decongestants taken by mouth.
Nonsteroidal anti-inflammatory medicines you can get without a prescription might ease discomfort. These include ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve). Or try acetaminophen (Tylenol, others).
Self-care therapies
The Valsalva maneuver can help ease pressure. In the Valsalva maneuver, you gently blow the nose while pinching the nostrils. Keep the mouth closed.
Surgery
Surgery to treat airplane ear is rarely needed. Even severe injuries, such as a burst eardrum or torn membranes of the inner ear, usually heal on their own.
But, rarely, you might need an office procedure or surgery to treat airplane ear. In one such procedure, a surgeon makes a cut in the eardrum to even out the air pressure and drain fluid. This is called a myringotomy.
Preparing for your appointment
If you have severe pain or symptoms linked to airplane ear that don't get better with self-care, talk to a healthcare professional. You might then be referred to an ear, nose and throat (ENT) specialist.
What you can do
To get ready for your appointment, make a list of:
- Your symptoms and when they began.
- All medications, vitamins or other supplements you take, including doses.
- Questions to ask your healthcare professional.
Questions about airplane ear might include:
- Did my recent airplane travel likely cause my ear symptoms?
- What is the best treatment?
- Am I likely to have lasting problems?
- How can I keep this from happening again?
- Should I change my travel plans?
Be sure to ask all the questions you have about airplane ear.
What to expect from your doctor
Questions might include:
- How bad are your symptoms?
- Do you have allergies?
- Have you had a cold, sinus infection or ear infection recently?
- Have you had airplane ear before?
- In the past, was your airplane ear severe or long-lasting?
What you can do in the meantime
To treat pain, you might take a nonsteroidal anti-inflammatory drug, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve), or a pain reliever, such as acetaminophen (Tylenol, others).
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use