
Blocked tear duct
Conditions
Overview
When a tear duct is blocked, tears can't drain in the usual way, causing the eye to be watery and irritated. The condition is caused by a partial or complete blockage in the tear drainage system.
A blocked tear duct is common in newborns. The condition usually gets better without any treatment during the first year of life. In adults, a blocked tear duct may be due to an injury, an infection or, rarely, a tumor.
A blocked tear duct can almost always be treated. Treatment depends on the cause of the blockage and the age of the affected person.
Symptoms
Symptoms of a blocked tear duct include:
- Very watery eye.
- Redness of the white part of the eye
- Eye infection or irritation that happens again and again, known as pink eye.
- Painful swelling near the inside corner of the eye.
- Crusting of the eyelids.
- Mucus or pus discharge from the lids and surface of the eye.
- Blurred vision.
When to see a doctor
See a healthcare professional if your eye tears constantly for several days or if your eye is infected often or all the time. A blocked tear duct may be caused by a tumor pressing on the tear drainage system. Finding the tumor early can give you more treatment options.
Causes
Blocked tear ducts can happen at any age, from birth to adulthood. Causes include:
- Blockage at birth. Many infants are born with blocked tear ducts. The tear drainage system may not be fully developed or there may be a problem with a duct. Often, a thin tissue membrane remains over the opening that empties into the nose, called the nasolacrimal duct.
- Age-related changes. As people age, the tiny openings that drain tears, called puncta, may get narrower, causing blockage.
- Infection or inflammation. Long-standing infection or inflammation of the eyes, tear drainage system or nose can cause the tear ducts to become blocked.
- Injury or trauma. An injury to the face can cause bone damage or scarring near the drainage system. This can affect the typical flow of tears through the ducts. Even small particles of dirt or loose skin cells lodged in the duct can cause blockage.
- Tumor. A tumor in the nose or anywhere along the tear drainage system can cause blockage.
- Eye drops. Rarely, long-term use of certain medicines, such as eye drops used to treat glaucoma, can cause a blocked tear duct.
- Cancer treatments. A blocked tear duct is a possible side effect of chemotherapy medicine and radiation treatment for cancer.
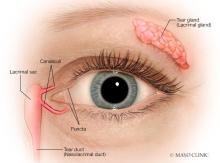
How the tear drainage system works
The lacrimal glands produce most of the eyes' tears. These glands are located inside the upper lids above each eye. Typically, tears flow from the lacrimal glands over the surface of the eye. Tears drain into openings called puncta on the inside corners of the upper and lower eyelids.
The puncta lead to small canals called canaliculi. Canaliculi move tears to a sac on the side of the nose called the lacrimal sac. From there, tears travel down the nasolacrimal duct and drain into the nose. Once in the nose, tears are absorbed again.
A blockage can happen at any point in the tear drainage system, from the puncta to the nose. When that happens, tears don't drain properly, causing watery eyes and increasing the risk of eye infections and irritation.
Risk factors
Certain factors increase the risk of developing a blocked tear duct:
- Age. Older adults are at increased risk of developing blocked tear ducts due to age-related changes.
- Ongoing eye inflammation. If the eyes are constantly irritated, red and inflamed, there is a higher risk of developing a blocked tear duct.
- Previous surgery. Previous eye, eyelid, nasal or sinus surgery may cause scarring of the duct system, possibly resulting in a blocked tear duct later.
- Glaucoma. Antiglaucoma medicines are often used on the surface of the eye. Medicines like these are called topical medicines. If you've used antiglaucoma or other topical eye medicines, you're at higher risk of developing a blocked tear duct.
- Previous cancer treatment. If you've had radiation or chemotherapy to treat cancer, particularly if the radiation was focused on your face or head, you're at higher risk of developing a blocked tear duct.
Complications
Because tears aren't draining the way they should, the tears that remain in the drainage system become stagnant. This promotes growth of bacteria, viruses and fungi, which can lead to frequent eye infections and inflammation.
Any part of the tear drainage system, including the clear membrane over the eye surface, known as the conjunctiva, can become infected or inflamed because of a blocked tear duct.
Diagnosis
To diagnose a blocked tear duct, a healthcare professional typically asks about symptoms, examines the eyes and does a few tests. The inside of the nose may be checked to see if any structural changes in the nasal passages are causing a blockage. If a blocked tear duct is suspected, other tests may be done to find the location of the blockage.
Tests used to diagnose a blocked tear duct include:
- Tear drainage test. This test measures how quickly tears are draining. One drop of a special dye is placed on the surface of each eye. If most of the dye is still on the surface of the eye after five minutes, a blocked tear duct may be diagnosed.
- Irrigation and probing. A saline solution may be flushed through the tear drainage system to check how well it's draining. Or a slender instrument may be inserted through the tiny drainage holes at the corner of the lid, called puncta, to check for blockages. In some people, this probing may even treat the condition.
- Eye imaging tests. For these procedures, a contrast dye is passed from the puncta in the corner of the lid through the tear drainage system. Then an X-ray, a CT scan or an MRI is used to find the location and cause of the blockage.
Treatment
Treatment depends on what's causing the blocked tear duct. More than one approach may be needed to correct the issue.
- Medicines to fight infection. If infection is present, antibiotic eye drops or pills may be prescribed.
-
Watch-and-wait or massage. Babies born with a blocked tear duct often get better without any treatment. This can happen as the drainage system matures during the first few months of life. Often, a thin tissue membrane remains over the opening that empties into the nose, called the nasolacrimal duct. If your baby's blocked tear duct isn't improving, the baby's care team may teach you a special massage technique to help open the membrane.
If a facial injury has caused blocked tear ducts, a health professional may suggest waiting a few months to see if the condition improves as the injury heals. As the swelling goes down, the tear ducts may become unblocked on their own.
-
Dilation, probing and flushing. For infants, this technique is done under general anesthesia. The provider enlarges the punctal openings with a special dilation tool. A thin probe is then placed through the puncta and into the tear drainage system.
For adults with partially narrowed puncta, a care professional may widen the puncta with a small probe and then flush the tear duct. This is called irrigation. Irrigation is a simple outpatient procedure that often provides at least temporary relief.
- Stenting, also called intubation. This procedure is usually done using general anesthesia. A thin tube made of silicone or polyurethane is threaded through one or both puncta in the corner of the eyelid. These tubes then pass through the tear drainage system into the nose. A small loop of tubing stays visible in the corner of the eye, and the tubes are generally left in for about three months before they're removed. Possible complications include inflammation from the presence of the tube.
- Balloon catheter dilation. If other treatments haven't worked or the blockage returns, this procedure may be used. It's usually effective for infants and toddlers and also may be used in adults with a partial blockage. First, a general anesthetic is given. Then a tube called a catheter is threaded through the tear duct blockage in the nose. The tube holds a deflated balloon on the tip. The balloon is then inflated and deflated a few times to open the blockage.
- Tumor treatment. If a tumor is causing the blocked tear duct, treatment focuses on the cause of the tumor. Surgery may be done to remove the tumor, or a healthcare professional may recommend using other treatments to shrink it.
Surgery
The surgery that's commonly used to treat blocked tear ducts is called dacryocystorhinostomy (DAK-ree-oh-sis-toe-rye-nohs-tuh-me). This procedure opens the passageway for tears to drain out of the nose again. A general anesthetic may be given; or a local anesthetic may be used if the surgery is done as an outpatient procedure.
The steps in this procedure vary depending on the exact location and extent of the blockage as well as the surgeon's experience and preferences.
- External. With external dacryocystorhinostomy, the surgeon makes a cut on the side of the nose, close to the lacrimal sac. After connecting the lacrimal sac to the nasal cavity and placing a stent in the new passageway, the surgeon closes up the cut with a few stitches. The stent holds the passageway open.
- Endoscopic or endonasal. With this method, the surgeon uses a microscopic camera and other tiny instruments inserted through the nasal opening to the duct system. This method requires no cut so it leaves no scar. But the success rates aren't as high as those with the external procedure.
Following surgery, a nasal decongestant spray and eye drops may be used to prevent infection and reduce inflammation. After healing for 6 to 12 weeks, the stents can typically be removed.
Prevention
To reduce the risk of developing a blocked tear duct later in life, get prompt treatment of eye inflammation or infections. Follow these tips to avoid eye infections in the first place:
- Wash your hands thoroughly and often.
- Try not to rub your eyes.
- Replace your eyeliner and mascara regularly. Never share these cosmetics with others.
- If you wear contact lenses, keep them clean according to recommendations provided by the manufacturer and your eye care specialist.
Preparing for your appointment
You may start by seeing someone on your primary healthcare team. You may then be referred to a doctor who specializes in treating conditions of the eye, called an ophthalmologist. In some instances, you may be referred to someone who specializes in plastic surgery for the eye.
Here's some information to help you get ready for your appointment.
What you can do
Before your appointment make a list of:
- Symptoms you've been having, including any that may not seem related to the reason for which you scheduled the appointment.
- All medicines, vitamins and supplements you take, including doses.
- Any eye drops that you've been taking.
- Questions to ask during the appointment.
For a blocked tear duct, some basic questions to ask include:
- What's the most likely cause of my symptoms?
- Are there other possible causes?
- Do I need any tests?
- How long will my condition last?
- What treatments are available, and which do you recommend?
- What side effects can I expect from treatment?
- Is this condition related to another medical condition?
- If I don't have any treatment, what are the risks to my vision?
- Do you have any brochures or other printed material that I can take with me? What websites do you recommend?
What to expect from your doctor
You'll likely be asked a few questions, such as:
- When did your symptoms begin?
- Do you have symptoms all the time, or do they come and go?
- Does anything ease your symptoms?
- Have you used any eye drops for this condition?
- Have you had any previous surgery to your eyes or eyelid?
- Have you had facial trauma, injuries, radiation treatment or surgery?
- Have you ever had any facial nerve conditions, such as Bell's palsy?
- Do you have other medical conditions, such as diabetes, or long-standing skin conditions, such as atopic dermatitis?
- Have you ever been diagnosed with a thyroid condition?
- Do you use contact lenses? Have you used contacts in the past?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use