
Cirrhosis
Conditions
Overview
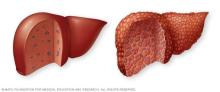
Cirrhosis is a complication of long-term inflammation of the liver. It results in the replacement of healthy liver tissue with scar tissue, called fibrosis. While heavy long-term alcohol use is a common cause of cirrhosis, many other diseases and liver conditions can lead to cirrhosis.
The definition of cirrhosis covers a broad process. As the liver is continually injured — whether by alcohol use, obesity or ongoing infection — it tries to repair itself. In the process, scar tissue forms. As cirrhosis gets worse, more and more scar tissue forms, making it difficult for the liver to do its job. Advanced cirrhosis is life-threatening.
The liver damage caused by cirrhosis generally can't be undone. But if liver cirrhosis is diagnosed early and the underlying cause is treated, further damage can be limited. In rare cases, it may be reversed.
Symptoms
Cirrhosis often has no symptoms until liver damage is serious. When symptoms do happen, they may include:
- Extreme tiredness.
- Easily bleeding or bruising.
- Loss of appetite.
- Nausea.
- Swelling in the legs, feet or ankles, called edema.
- Weight loss.
- Itchy skin.
- Yellowing of the skin and eyes, called jaundice.
- Fluid buildup in the belly, called ascites (uh-SY-teez).
- Spiderlike blood vessels on the skin, called spider angiomas.
- Redness in the palms of the hands.
- Pale fingernails, especially the thumb and index finger.
- Clubbing of the fingers, in which the fingertips spread out and become rounder than usual.
- Confusion, drowsiness or slurred speech.
Sexual problems may affect both men and women with cirrhosis. In men, erectile dysfunction, loss of sex drive and shrinkage of the testicles are common. A type of breast enlargement called gynecomastia also may occur.
In women, low sex drive, painful intercourse, inability to reach orgasm and lack of ovulation may occur. Women also may lose their periods, even when they're not in menopause.
When to see a doctor
Make an appointment with a healthcare professional if you have any of the symptoms noted above.
Causes
A wide range of diseases and conditions can damage the liver and lead to cirrhosis.
Some of the causes include:
- Long-term alcohol use disorder.
- Viral hepatitis (hepatitis B and hepatitis C).
- Metabolic dysfunction-associated steatotic liver disease — formerly known as nonalcoholic fatty liver disease or NASH cirrhosis — a condition in which fat builds up in the liver.
- Hemochromatosis, which is a condition that causes iron buildup in the body.
- Autoimmune hepatitis, which is a liver disease caused by the body's immune system.
- Destruction of the bile ducts caused by primary biliary cholangitis.
- Hardening and scarring of the bile ducts caused by primary sclerosing cholangitis.
- Wilson's disease — a condition in which copper builds up in the liver.
- Cystic fibrosis, which is a condition that damages the lungs, digestive system and other organs.
- Alpha-1-antitrypsin deficiency, which is a condition that damages the lungs, liver, skin and blood vessels.
- Poorly formed bile ducts — a condition known as biliary atresia.
- Diseases of sugar metabolism, such as galactosemia or glycogen storage disease.
- Alagille syndrome, which is a genetic digestive disorder.
- Infection, such as syphilis or brucellosis.
- Medicines, including methotrexate or isoniazid.
Risk factors
- Drinking alcohol. Alcohol use is a risk factor for cirrhosis.
- Being overweight. Being obese increases the risk of conditions that may lead to cirrhosis. These conditions include metabolic dysfunction-associated steatotic liver disease, formerly called nonalcoholic fatty liver disease, and metabolic dysfunction-associated steatohepatitis, formerly called nonalcoholic steatohepatitis.
- Having viral hepatitis. Not everyone with chronic hepatitis will develop cirrhosis, but it's one of the world's leading causes of liver disease.
Complications
Complications of cirrhosis usually mean the liver disease has become more advanced. When complications develop, they increase the risk of serious illness and may signal a higher chance of death compared with earlier stages of cirrhosis.
- High blood pressure in the veins that supply the liver. Cirrhosis can raise pressure in the veins that carry blood through the liver, a condition called portal hypertension. This increased pressure can lead to serious complications, including ascites and bleeding.
- Swelling in the legs and belly. The increased pressure in the portal vein can cause fluid to build up in the legs, called edema, and in the belly, called ascites. Edema and ascites also may happen if the liver can't make enough of certain blood proteins, such as albumin. Once ascites develops, the risk of further complications increases.
- Swelling of the spleen. Portal hypertension can cause the spleen to trap white blood cells and platelets. This makes the spleen swell. This condition is known as splenomegaly. Fewer white blood cells and platelets in your blood can be the first sign of cirrhosis.
- Bleeding. Portal hypertension can cause blood to be redirected to smaller veins. Strained by the extra pressure, these smaller veins can burst, causing serious bleeding. Portal hypertension also may cause enlarged veins, called varices (VAR-ih-sees), in the esophagus or the stomach. Enlarged veins in the esophagus increase the risk of serious bleeding, which can be life-threatening. If the liver can't make enough clotting factors, this also can contribute to continued bleeding.
- Broken blood vessels. Blood vessels under the skin may break, creating patterns that look like spiders. These blood vessels are called spider angiomas.
- Infections. Having cirrhosis makes it hard for the body to fight infections. Ascites also can lead to bacterial peritonitis, an infection of fluid in the belly. This is a serious infection that can trigger kidney failure and other organ problems.
- Malnutrition. Cirrhosis may make it more difficult for the body to process nutrients, leading to weakness and weight loss.
- Buildup of toxins in the brain. A liver damaged by cirrhosis can't clear toxins from the blood as well as a healthy liver can. These toxins can then build up in the brain and cause mental confusion and difficulty concentrating. This is known as hepatic encephalopathy. This is a sign of advanced cirrhosis. Over time, it can progress to unresponsiveness or coma.
- Jaundice. Jaundice happens when the diseased liver doesn't remove enough of a blood waste product, called bilirubin, from the blood. Jaundice causes yellowing of the skin and whites of the eyes and darkening of urine. When jaundice develops in cirrhosis, it is a sign of worsening liver function.
- Kidney failure. Cirrhosis can reduce blood flow to the kidneys and lead to kidney failure, sometimes called hepatorenal syndrome.
- Bone disease. Some people with cirrhosis lose bone strength and are at greater risk of fractures.
- Increased risk of liver cancer. A large proportion of people who develop liver cancer have preexisting cirrhosis.
- Acute-on-chronic cirrhosis. Some people end up having multiorgan failure. Researchers now believe this is a complication in some people who have cirrhosis. However, they don't fully understand what causes it.
When jaundice, ascites, bleeding, liver cancer or brain changes occur, healthcare professionals may call the condition decompensated cirrhosis. Without these complications cirrhosis is said to be compensated.
Prevention
Lower the risk of cirrhosis by taking these steps to care for your liver:
- Do not drink alcohol. If you have liver disease, you should not consume any kind of alcoholic drink, even if alcohol was not the original cause.
- Eat a healthy diet. Choose a diet that's full of fruits and vegetables. Select whole grains and lean sources of protein. Cut down on the amount of fatty and fried foods you eat.
- Maintain a healthy weight. Too much body fat can damage the liver. Talk to a healthcare professional about a weight-loss plan if you carry excess weight.
- Reduce your risk of hepatitis. Sharing needles and having unprotected sex can increase the risk of hepatitis B and C. Ask a health professional about hepatitis vaccinations. Hepatitis C can be cured. All adults should be screened for hepatitis C at least once.
If you're concerned about your risk of liver cirrhosis, talk to a health professional about ways to reduce your risk.
Diagnosis
People with early-stage cirrhosis of the liver usually don't have symptoms. Often, cirrhosis is first noticed during a blood test or checkup for another reason. To help confirm a diagnosis, a combination of laboratory and imaging tests is usually done.
Tests
A healthcare professional may order one or more tests to check liver function, including:
-
Lab tests. A healthcare professional may order blood tests to check for signs of liver malfunction, such as high bilirubin levels or certain enzymes. To evaluate kidney function, the blood is checked for creatinine. A blood count would be measured and blood is screened for hepatitis viruses. An international normalized ratio (INR), also called prothrombin test, is checked for the blood's ability to clot. Together, the results of such tests show the presence of cirrhosis.
A healthcare professional may be able to diagnose the underlying cause of cirrhosis based on your medical history and blood test results. Blood tests also can help show how severe the liver disease is and how it changes over time.
Health professionals sometimes use the information from blood tests to calculate what's called a model for end-stage liver disease (MELD) score. The MELD score can help assess liver function and guide monitoring and treatment decisions. A higher MELD score means liver function is worsening and closer monitoring or advanced care may be needed. Health professionals often track the MELD score over time to help decide when to consider referral to a liver specialist or transplant center.
The MELD score is only one part of the evaluation of cirrhosis. Health professionals also consider symptoms, complications such as fluid buildup or confusion, and overall health when assessing cirrhosis severity.
-
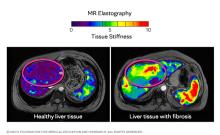
Imaging tests. Certain imaging tests, including transient or magnetic resonance elastography (MRE), may be recommended. These noninvasive imaging tests look for hardening or stiffening of the liver. When a liver biopsy may have been necessary in years past, MRE may provide the same information with less discomfort and risk.
Other imaging tests, such as MRI, CT and ultrasound, also may be done.
- Biopsy. A tissue sample, called a biopsy, is not necessarily needed for diagnosis, particularly with the widespread availability of magnetic resonance elastography. But a biopsy is sometimes still needed in certain situations.
Ongoing monitoring
If you have cirrhosis, a healthcare professional is likely to recommend regular tests to see if liver disease has progressed or check for signs of complications, especially esophageal varices and liver cancer. Noninvasive tests are becoming more widely available for keeping an eye on liver disease.
Treatment
Treatment for cirrhosis depends on the cause and extent of liver damage. The goals of treatment are to slow the progression of scar tissue in the liver and to prevent or treat symptoms and complications of cirrhosis. Reversal of cirrhosis usually isn't possible. For severe liver damage, hospitalization may be needed.
Treatment for the underlying cause of cirrhosis
In early cirrhosis, it may be possible to minimize damage to the liver by treating the underlying cause. The options include:
- Treatment for alcohol dependency. People with cirrhosis caused by excessive alcohol use must stop drinking entirely. Any type and amount of alcohol is toxic to the liver. If stopping alcohol use is difficult, a healthcare professional may recommend a treatment program. Such a program is typically required for anyone considering liver transplantation. Stopping alcohol use can slow liver damage, lower the risk of complications and improve life expectancy in people with alcohol-related cirrhosis.
- Weight loss. People with cirrhosis caused by metabolic dysfunction-associated steatotic liver disease may become healthier if they lose weight and control their blood sugar levels.
- Medicines to control hepatitis. Medicines may limit further damage to liver cells caused by hepatitis B or C through specific treatment of these viruses.
- Medicines to control other causes and symptoms of cirrhosis. Medicines may slow the progression of certain types of liver cirrhosis. For example, for people with primary biliary cholangitis that is diagnosed early, medicine may significantly delay progression to cirrhosis.
Other medicines can relieve certain symptoms, such as itching, fatigue and pain. Nutritional supplements or vitamins may be prescribed to treat malnutrition associated with cirrhosis. Supplements also can help prevent weak bones, known as osteoporosis.
Making healthy lifestyle choices can help protect your liver and support overall health. These choices include following a balanced diet, being physically active as tolerated and taking steps to prevent infections. Your care team can help tailor self-care plans for your needs and may recommend specific nutrition advice, vaccinations and safe pain medicine options.
Treatment for complications of cirrhosis
A healthcare professional will work to treat any complications of cirrhosis, including:
- A buildup of fluid in the body. A low-sodium diet and medicine to prevent fluid buildup in the body may help control ascites and swelling. More-severe fluid buildup may need procedures to drain the fluid or surgery to relieve pressure.
-
Portal hypertension. Certain blood pressure medicines may control increased pressure in the veins that supply the liver, called portal hypertension, and prevent severe bleeding. An upper endoscopy may be done on a regular basis to look for enlarged veins in the esophagus or stomach that may bleed. These veins are known as varices.
If someone develops varices, medicine will likely be prescribed to lower the risk of bleeding. If there are signs that the varices are bleeding or are likely to bleed, a procedure known as band ligation may be needed. Band ligation can stop the bleeding or reduce the risk of further bleeding. In severe cases, a small tube called a transjugular intrahepatic portosystemic shunt may be placed in the vein to reduce blood pressure in the liver.
- Infections. Antibiotics or other treatments for infections may be needed. A healthcare professional also is likely to recommend vaccinations for influenza, pneumonia and hepatitis.
- Increased liver cancer risk. A healthcare professional will likely recommend regular blood tests and ultrasound exams to look for signs of liver cancer.
- Hepatic encephalopathy. Some people may be prescribed medicines to help reduce the buildup of toxins in the blood caused by poor liver function.
Liver transplant surgery
In advanced cases of cirrhosis, when the liver stops working properly, a liver transplant may be the only treatment option. A liver transplant is a procedure to replace the liver with a healthy liver from a deceased donor or with part of a liver from a living donor. Cirrhosis is one of the most common reasons for a liver transplant. Candidates for liver transplant have extensive testing to determine whether they are healthy enough to have a good outcome following surgery.
Historically, those with alcoholic cirrhosis have not been liver transplant candidates because of the risk that they will return to harmful drinking after transplant. But many people who are treated for alcohol use disorder and remain abstinent have post-transplant survival rates similar to those of liver transplant recipients with other types of liver disease.
For transplant to be an option if you have alcoholic cirrhosis, you will need to:
- Find a program that works with people who have alcoholic cirrhosis.
- Meet the requirements of the program. These would include lifelong commitment to alcohol abstinence as well as other requirements of the specific transplant center.
Potential future treatments
Scientists are working to expand current treatments for cirrhosis, but success has been limited. Because cirrhosis has a variety of causes and complications, there are many potential avenues of approach. A combination of increased screening, lifestyle changes and new medicines may improve outcomes for people with liver damage, if started early.
Researchers are working on therapies that will specifically target liver cells, helping to slow or even reverse the scarring, called fibrosis, that leads to cirrhosis. However, no targeted therapy is quite ready.
Prognosis
Cirrhosis is a serious condition, but it is not always immediately life-threatening. Many people live for years with cirrhosis, especially when it is found early and carefully managed. The disease becomes much more dangerous once the liver can no longer perform its basic functions and complications appear. Most deaths related to cirrhosis occur after the disease progresses to a more advanced stage.
How stage affects outlook
Healthcare professionals often describe cirrhosis as compensated or decompensated. These are clinical stages based on liver function and the presence of complications.
- Compensated cirrhosis. At this stage, the liver is scarred but still able to function. People often have few or no symptoms and may live for many years. On average, life expectancy is more than 10 years, especially when the cause of cirrhosis is treated and complications are prevented.
-
Decompensated cirrhosis. At this advanced stage, the liver can no longer meet the body's needs. This can cause problems, such as fluid buildup, bleeding, confusion or jaundice. Once cirrhosis becomes decompensated, average life expectancy drops to about two years without liver transplant. Many things can influence life expectancy for each person, including complications and treatment.
At this stage, care focuses on symptom control, preventing complications and discussing advanced care options, including liver transplant when appropriate.
What can change prognosis over time
Cirrhosis often develops slowly over many years, but progression is not the same for everyone. Factors that can speed disease progression include:
- Ongoing liver injury.
- Untreated viral hepatitis.
- Continued alcohol use.
- Serious infections or kidney problems.
These factors increase the risk of complications and worsening liver function.
Lifestyle and home remedies
If you have cirrhosis, be careful to limit additional liver damage:
- Don't drink alcohol. Whether your cirrhosis was caused by chronic alcohol use or another disease, don't drink alcohol. Drinking alcohol may cause further liver damage. This is true for all types of alcoholic drinks.
- Eat a low-sodium diet. Excess salt can cause your body to retain fluids, worsening swelling in your abdomen and legs. Use herbs for seasoning your food, rather than salt. Choose prepared foods that are low in sodium.
- Eat a healthy diet. People with cirrhosis can experience malnutrition. Combat this with a healthy diet that includes a variety of fruits and vegetables. Choose lean protein, such as legumes, poultry or fish. Don't eat raw seafood. Getting plenty of protein may help restore your health. Eating small meals often may make it easier to follow the diet from your care team.
- Protect yourself from infections. Cirrhosis makes it more difficult for you to fight off infections. Protect yourself by avoiding people who are sick and washing your hands frequently. Get vaccinated for hepatitis A and B, influenza, and pneumonia.
- Use over-the-counter medicines carefully. Cirrhosis makes it more difficult for your liver to process medicines. For this reason, ask a healthcare professional before taking any medicines, including nonprescription ones. Don't take aspirin and ibuprofen (Advil, Motrin IB, others). If you have liver damage, a care professional may recommend that you not take acetaminophen (Tylenol, others) or take it in low doses for pain relief.
Even with careful attention to diet and day-to-day habits, cirrhosis is a very serious condition that often shortens life. Your care team will tell you what you can do to stay as healthy as possible as long as possible.
Preparing for an appointment
If you have cirrhosis, you may be referred to a healthcare professional who specializes in the digestive system, called a gastroenterologist, or the liver, called a hepatologist.
Here's some information to help you get ready for your appointment and what to expect.
What you can do
- Be aware of any pre-appointment restrictions, such as diet restrictions on the day before your appointment.
- Write down your symptoms, including when they started and how they may have changed or worsened over time.
- Take a list of all your medicines, as well as any vitamins or supplements, including the doses.
- Write down your key medical information, including other diagnosed conditions.
- Bring results of medical tests done so far, including digital copies of CT, MRI, or ultrasound images and biopsy slides if a liver biopsy has been done.
- Write down key personal information, including any recent changes or stressors in your life.
- Take a family member or friend along to help you remember things.
- Write down questions to ask your doctor.
Questions to ask your doctor
Preparing a list of questions can help you make the most of your time. Some basic questions to ask include:
- What is most likely causing my cirrhosis?
- Is there a way to slow or stop my liver damage?
- What are my treatment options?
- Are there medicines or supplements that can hurt my liver?
- What signs and symptoms of complications should I watch for?
- I have other health conditions. How can I best manage them together?
Don't hesitate to ask additional questions during your appointment.
What to expect from your doctor
Be prepared to answer questions, including:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- How often do you drink alcohol?
- Have you been exposed to or taken toxic drugs?
- Do you have a family history of liver disease, hemochromatosis or obesity?
- Have you ever had viral hepatitis?
- Have you ever had jaundice?
- Have you ever had a blood transfusion or used injected drugs?
- Do you have any tattoos?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use