
Fetal macrosomia
Conditions
Overview
Fetal macrosomia is a condition in which an unborn baby, called a fetus, is much larger than average.
A fetus diagnosed with fetal macrosomia is estimated to weigh more than 8 pounds, 13 ounces (4,000 grams) at any stage of pregnancy. Fetal macrosomia affects about 9% of babies worldwide. The health risks linked to fetal macrosomia go up greatly when a fetus weighs more than 9 pounds, 15 ounces (4,500 grams).
Fetal macrosomia may lead to health concerns for a pregnant person during a vaginal delivery. It also can put a fetus at risk of injury during childbirth. Fetal macrosomia puts a baby at a higher risk of some health issues after birth too.
Symptoms
Fetal macrosomia can be hard to find and identify during pregnancy. Symptoms include the following.
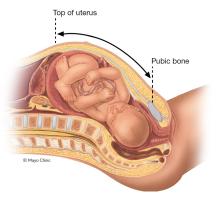
Large fundal height
During prenatal visits, the distance from the top of the uterus to the pubic bone often is measured. This is called fundal height. A larger than expected fundal height could be a sign of fetal macrosomia.
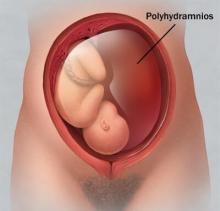
Too much amniotic fluid
The fluid that surrounds and protects a fetus during pregnancy is called amniotic fluid. Having more of this fluid than usual might be a sign that a fetus is larger than average. In part, that's because a fetus's urine contributes to the amniotic fluid. And a larger fetus makes more urine. Some health conditions that cause a fetus to be larger also might raise the amount of urine the fetus makes. The medical term for having extra amniotic fluid is polyhydramnios.
Causes
Genetic factors and health conditions that affect a pregnant person, such as obesity or diabetes, can cause fetal macrosomia. Rarely, a medical condition in a fetus might make the fetus grow faster and larger than is typical. Sometimes the cause of fetal macrosomia is not known.
Risk factors
Many factors can raise the risk of fetal macrosomia. Examples include:
-
Diabetes. Fetal macrosomia is more likely when a pregnant person has diabetes. That's true whether the diabetes existed before pregnancy, called pregestational diabetes, or if it develops during pregnancy, called gestational diabetes.
If diabetes isn't well managed in a pregnant person, a fetus is likely to develop larger shoulders and more body fat.
- Obesity. Fetal macrosomia is more likely in pregnant people who have obesity.
- Extra weight gain. Gaining too much weight during pregnancy raises the risk of fetal macrosomia.
- A history of fetal macrosomia. People who have given birth to a large baby before are at higher risk of having another large baby. Also, pregnant people who weighed more than 8 pounds, 13 ounces at birth are more likely to give birth to a large baby.
- Overdue pregnancy. If pregnancy goes more than a week past the due date, a baby is at higher risk of fetal macrosomia.
- Previous pregnancies. The risk of fetal macrosomia goes up with each pregnancy.
- Age. Pregnant people older than 35 are more likely to have a baby with fetal macrosomia.
Fetal macrosomia is more likely to be a result of diabetes, obesity or extra weight gain during pregnancy than other causes.
Complications
Fetal macrosomia poses a number of health risks, called complications, for the pregnant person and the fetus. Some of these issues also can affect a baby's health after birth.
Risks during labor and delivery
Possible health concerns of fetal macrosomia during labor and delivery include the following.
-
Difficult labor. A large fetus can make childbirth harder. For example, during delivery fetal macrosomia can cause:
- A baby to become stuck in the birth canal, a condition called shoulder dystocia.
- Injuries to the baby during childbirth.
- Delivery with forceps or a vacuum device. This is called operative vaginal delivery.
- A C-section to be more likely.
- Birth canal injuries. During childbirth, fetal macrosomia can cause tissue in the vagina to tear. The muscles between the vagina and the anus, called the perineal muscles, also may tear. These tears are called genital tract lacerations.
- Bleeding after delivery. Fetal macrosomia raises the risk that uterine muscles won't properly contract after childbirth. That condition is called uterine atony. If the uterus doesn't contract as it should, that could lead to serious bleeding after delivery.
- Uterine rupture. For a pregnant person who has had a C-section before or has had major uterine surgery, fetal macrosomia raises the risk of uterine rupture during labor. This is a rare but serious health concern in which the uterus tears open along the scar from a C-section or other surgery. If this happens, an emergency C-section is needed to prevent health problems that could be life-threatening.
Risks for the baby after birth
Possible health concerns after the baby is born that are linked to fetal macrosomia include:
- Trouble breathing.
- Low blood sugar, called hypoglycemia.
- A blood condition that results in a high red blood cell count, called polycythemia.
Babies born with fetal macrosomia also are at higher risk of several other health concerns as they grow, including:
- Obesity.
- Diabetes and other conditions linked to difficulty managing blood sugar.
- Some forms of heart disease.
- Metabolic syndrome. This is a group of conditions that happen together. They include high blood pressure, high blood sugar, extra body fat around the waist, and cholesterol levels that are not in the healthy range.
Prevention
It may not be possible to prevent fetal macrosomia. But taking the following steps to promote a healthy pregnancy could lower the risk of macrosomia.
Talk with a healthcare professional first
If possible, make an appointment to see a healthcare professional before you get pregnant. At the appointment, talk about your health history and other factors that could affect a pregnancy. If obesity is a concern, it may be useful to work with a registered dietitian or an obesity specialist or both. They may be able to help you find ways to reach a healthy weight before pregnancy.
Be active
Research shows that exercising during pregnancy can lower the risk of fetal macrosomia. Talk with your healthcare professional about the physical activity that's best for you.
Gain pregnancy weight carefully
Gain a healthy amount of weight during pregnancy. Typically, that's about 25 to 35 pounds (about 11 to 16 kilograms) for people who are at a healthy weight before pregnancy. People who weigh more when they get pregnant may need to gain less weight. Work with your healthcare professional to decide what's right for you.
Manage diabetes
If you have diabetes, work with your healthcare professional to manage the condition. Keeping blood sugar within a healthy range is one of best ways to prevent health concerns during pregnancy, including fetal macrosomia.
Diagnosis
Fetal macrosomia can't be definitively diagnosed until after a baby is born and weighed.
But if you have risk factors for fetal macrosomia, your healthcare professional likely will use tests to monitor your pregnancy. They may include the following tests.
Ultrasound
Toward the end of the third trimester, you may have an ultrasound. During that test, parts of the fetus's body are measured, such as the head, belly and legs. Those measurements can be used to estimate fetal weight. But the accuracy of ultrasound for predicting fetal macrosomia is not always reliable.
Ongoing tests during pregnancy
If fetal macrosomia is suspected due to a health condition in a pregnant person, such as diabetes, several tests may be recommended throughout pregnancy to watch a fetus's health. This is called antenatal testing. These tests typically aren't done when only fetal macrosomia is suspected, and there are no other health concerns.
The tests may include:
- Nonstress test. A nonstress test measures how fetal heart rate changes in response to a fetus's movements.
- Fetal biophysical profile. A fetal biophysical profile combines a nonstress test with ultrasound. It checks a fetus's movement and breathing, as well as the amount of amniotic fluid.
If there's a risk of fetal macrosomia, it can be helpful to talk with a doctor who specializes in caring for children, called a pediatrician, who has expertise in treating babies with fetal macrosomia.
Treatment
Even when a fetus is large, vaginal delivery may be possible. Before labor begins, talk with your healthcare professional about your options as well as risks and benefits.
Triggering uterine contractions with medicine before labor begins on its own, called inducing labor, typically isn't advised for fetal microsomia unless there are other health conditions that make inducing labor necessary. Research suggests that labor induction doesn't lower the risk of health concerns linked to fetal macrosomia.
A C-section might be recommended in the following situations:
- A pregnant person has diabetes, and a fetus is estimated to weigh 9 pounds, 15 ounces (4,500 grams) or more.
- A pregnant person doesn't have diabetes, and a fetus is estimated to weigh 11 pounds (5,000 grams) or more.
- A pregnant person has delivered a baby whose shoulder got stuck behind the pelvic bone in an earlier pregnancy. That condition is called shoulder dystocia.
If your healthcare professional suggests a C-section, make sure you understand the risks and benefits.
After a baby with fetal macrosomia is born, the baby likely will be examined for:
- Signs of birth injuries.
- Low blood sugar, called hypoglycemia.
- A blood condition that results in a high red blood cell count, called polycythemia.
The baby might need special care in a neonatal intensive care unit.
A baby with fetal microsomia may be at risk of childhood obesity and diabetes. Talk with your baby's healthcare professional about regularly checking for those conditions as the child grows.
If you give birth to a baby with fetal macrosomia and you haven't been diagnosed with diabetes before, you may be tested for diabetes. During future pregnancies, it's likely you'll be watched closely for symptoms of gestational diabetes. That's a type of diabetes that develops during pregnancy.
Coping and support
If your healthcare professional suspects fetal macrosomia during your pregnancy, you might feel anxious and worried.
Talk with your healthcare professional about what you can do to ease stress and promote a healthy pregnancy. You also may want to talk with others who've had babies with fetal macrosomia. Ask a member of your healthcare team about support groups and other resources that may be available in your area or online.
Preparing for your appointment
If you have risk factors for fetal macrosomia, the topic is likely to come up during your prenatal appointments.
Below are some questions to ask your healthcare professional about fetal macrosomia:
- What is the likely cause of the condition?
- What tests do I need?
- What needs to be done now?
- Do I need to follow any restrictions?
- How will fetal macrosomia affect my baby?
- Will I need to have a C-section?
- Will my baby need tests or special care after delivery?
If you think of other questions during the appointment, be sure to ask them too.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use