
Gastroesophageal reflux disease (GERD)
Conditions
Overview
Gastroesophageal reflux disease happens when stomach acid flows back up into the esophagus and causes heartburn. It's often called GERD for short. This backwash is known as acid reflux, and it can irritate the lining of the esophagus.
Many people experience acid reflux now and then. However, when acid reflux happens repeatedly over time, it can cause GERD.
Most people can manage the discomfort of GERD with lifestyle changes and medicines. And though it's uncommon, some may need surgery to help with symptoms.
Symptoms
Common symptoms of GERD include:
- A burning sensation in the chest, often called heartburn. Heartburn usually happens after eating and might be worse at night or while lying down.
- Backwash of food or sour liquid in the throat.
- Upper belly or chest pain.
- Trouble swallowing, called dysphagia.
- Sensation of a lump in the throat.
If you have nighttime acid reflux, you also might experience:
- An ongoing cough.
- Inflammation of the vocal cords, known as laryngitis.
- New or worsening asthma.
When to see a doctor
Seek medical help right away if you have chest pain, especially if you also have shortness of breath, or jaw or arm pain. These may be symptoms of a heart attack.
Make an appointment with a healthcare professional if you:
- Have severe or frequent GERD symptoms.
- Take nonprescription medicines for heartburn more than twice a week.
Causes
GERD is caused by frequent acid reflux or reflux of nonacidic content from the stomach.
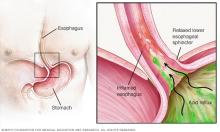
When you swallow, a circular band of muscle around the bottom of the esophagus, called the lower esophageal sphincter, relaxes to allow food and liquid to flow into the stomach. Then the sphincter closes again.
If the sphincter does not relax as is typical or it weakens, stomach acid can flow back into the esophagus. This constant backwash of acid irritates the lining of the esophagus, often causing it to become inflamed.
Risk factors
Conditions that can increase the risk of GERD include:
- Obesity.
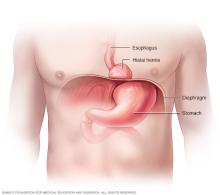
- Bulging of the top of the stomach up above the diaphragm, known as a hiatal hernia.
- Pregnancy.
- Connective tissue disorders, such as scleroderma.
- Delayed stomach emptying.
Factors that can aggravate acid reflux include:
- Smoking.
- Eating large meals or eating late at night.
- Eating certain foods, such as fatty or fried foods.
- Drinking certain beverages, such as alcohol or coffee.
- Taking certain medicines, such as aspirin.
Complications
Over time, long-lasting inflammation in the esophagus can cause:
- Inflammation of the tissue in the esophagus, known as esophagitis. Stomach acid can break down tissue in the esophagus. This can cause inflammation, bleeding and sometimes an open sore, called an ulcer. Esophagitis can cause pain and make swallowing difficult.
- Narrowing of the esophagus, called an esophageal stricture. Damage to the lower esophagus from stomach acid causes scar tissue to form. The scar tissue narrows the food pathway, leading to problems with swallowing.
- Precancerous changes to the esophagus, known as Barrett esophagus. Damage from acid can cause changes in the tissue lining the lower esophagus. These changes are associated with an increased risk of esophageal cancer.
Diagnosis
A healthcare professional might be able to diagnose GERD based on a history of symptoms and a physical examination.
To confirm a diagnosis of GERD, or to check for complications, a care professional might recommend:
-
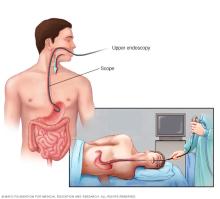
Upper endoscopy. An upper endoscopy uses a tiny camera on the end of a flexible tube to visually examine the upper digestive system. The camera helps provide a view of the inside of the esophagus and stomach. Test results may not show when reflux is present, but an endoscopy may find inflammation of the esophagus or other complications.
An endoscopy also can be used to collect a sample of tissue, called a biopsy, to be tested for complications such as Barrett esophagus. In some instances, if a narrowing is seen in the esophagus, it can be stretched or dilated during this procedure. This is done to improve trouble swallowing.
-
Ambulatory acid (pH) probe test. A monitor is placed in the esophagus to identify when, and for how long, stomach acid regurgitates there. The monitor connects to a small computer that's worn around the waist or with a strap over the shoulder.
The monitor might be a thin, flexible tube, called a catheter, that's threaded through the nose into the esophagus. Or it might be a clip that's placed in the esophagus during an endoscopy. The clip passes into the stool after about two days.
-
X-ray of the upper digestive system. X-rays are taken after drinking a chalky liquid that coats and fills the inside lining of the digestive tract. The coating allows a healthcare professional to see a silhouette of the esophagus and stomach. This is particularly useful for people who are having trouble swallowing.
Sometimes, an X-ray is done after swallowing a barium pill. This can help diagnose a narrowing of the esophagus that's interfering with swallowing.
- Esophageal manometry. This test measures the rhythmic muscle contractions in the esophagus while swallowing. Esophageal manometry also measures the coordination and force exerted by the muscles of the esophagus. This is typically done in people who have trouble swallowing.
- Transnasal esophagoscopy. This test is done to look for any damage in the esophagus. A thin, flexible tube with a video camera is put through the nose and moved down the throat into the esophagus. The camera sends pictures to a video screen.
Treatment

A healthcare professional is likely to recommend trying lifestyle changes and nonprescription medicines as a first line of treatment. If you don't experience relief within a few weeks, prescription medicine and additional testing may be recommended.
Nonprescription medicines
Options include:
- Antacids that neutralize stomach acid. Antacids containing calcium carbonate, such as Mylanta, Rolaids and Tums, may provide quick relief. But antacids alone won't heal an inflamed esophagus damaged by stomach acid. Overuse of some antacids can cause side effects, such as diarrhea or sometimes kidney complications.
- Medicines to reduce acid production. These medicines — known as histamine (H-2) blockers — include cimetidine (Tagamet HB), famotidine (Pepcid AC) and nizatidine (Axid). H-2 blockers don't act as quickly as antacids, but they provide longer relief and may decrease acid production from the stomach for up to 12 hours. Stronger versions are available by prescription.
- Medicines that block acid production and heal the esophagus. These medicines — known as proton pump inhibitors — are stronger acid blockers than H-2 blockers and allow time for damaged esophageal tissue to heal. Nonprescription proton pump inhibitors include lansoprazole (Prevacid), omeprazole (Prilosec OTC) and esomeprazole (Nexium).
If you start taking a nonprescription medicine for GERD, be sure to inform your care provider.
Prescription medicines
Prescription-strength treatments for GERD include:
-
Prescription-strength proton pump inhibitors. These include esomeprazole (Nexium), lansoprazole (Prevacid), omeprazole (Prilosec), pantoprazole (Protonix), rabeprazole (Aciphex) and dexlansoprazole (Dexilant).
Although generally well tolerated, these medicines might cause diarrhea, headaches, nausea or, in rare instances, low vitamin B-12 or magnesium levels.
- Prescription-strength H-2 blockers. These include prescription-strength famotidine and nizatidine. Side effects from these medicines are generally mild and well tolerated.
- Potassium-competitive acid blockers (P-CABs). This new class of medicines may be recommended for someone with severe acid reflux if other medicines haven't worked. They include vonoprazan (Voquezna) and tegoprazan (K-Cab).
Deep-breathing training
A technique known as diaphragmatic breathing may help improve GERD symptoms for some people. This exercise is done after eating. It involves breathing deeply into the diaphragm rather than shallowly into the chest. Diaphragmatic breathing techniques should ideally be taught by a trained medical professional.
Surgery and other procedures
GERD can usually be controlled with medicine. But if medicines don't help or you wish to avoid long-term medicine use, a healthcare professional might recommend:
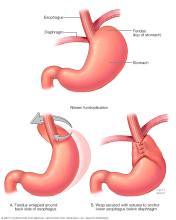
- Fundoplication. The surgeon wraps the top of the stomach around the lower esophageal sphincter, to tighten the muscle and prevent reflux. Fundoplication is usually done with a minimally invasive, called laparoscopic, procedure. The wrapping of the top part of the stomach can be partial or complete, known as Nissen fundoplication. The most common partial procedure is the Toupet fundoplication. Your surgeon typically recommends the type that is best for you.
- LINX device. A ring of tiny magnetic beads is wrapped around the junction of the stomach and esophagus. The magnetic attraction between the beads is strong enough to keep the junction closed to refluxing acid, but weak enough to allow food to pass through. The LINX device can be implanted using minimally invasive surgery. The magnetic beads do not affect airport security or magnetic resonance imaging.
-
Transoral incisionless fundoplication (TIF). This new procedure involves tightening the lower esophageal sphincter by creating a partial wrap around the lower esophagus using polypropylene fasteners. TIF is performed through the mouth by using an endoscope and requires no surgical incision. Its advantages include quick recovery time and high tolerance.
If you have a large hiatal hernia, TIF alone is not an option. However, TIF may be possible if it is combined with laparoscopic hiatal hernia repair.
Because obesity can be a risk factor for GERD, a healthcare professional could suggest weight-loss surgery as an option for treatment. Talk with your healthcare team to find out if you're a candidate for this type of surgery.
Emerging therapies
Lifestyle and home remedies
Lifestyle changes may help reduce the frequency of acid reflux. Try to:
- Maintain a healthy weight. Excess pounds put pressure on the abdomen, pushing up the stomach and causing acid to reflux into the esophagus.
- Stop smoking. Smoking decreases the lower esophageal sphincter's ability to function properly.
- Elevate the head of your bed. If you regularly experience heartburn while trying to sleep, place wood or cement blocks under the feet at the head end of your bed. Raise the head end by 6 to 9 inches. If you can't elevate your bed, you can insert a wedge between your mattress and box spring to elevate your body from the waist up. Raising your head with additional pillows isn't effective.
- Start on your left side. When you go to bed, start by lying on your left side to help make it less likely to have reflux.
- Don't lie down after a meal. Wait at least three hours after eating before lying down or going to bed.
- Eat food slowly and chew thoroughly. Put down your fork after every bite and pick it up again once you have chewed and swallowed that bite.
- Don't consume foods and drinks that trigger reflux. Common triggers include alcohol, chocolate, caffeine, fatty foods or peppermint.
- Don't wear tight-fitting clothing. Clothes that fit tightly around the waist put pressure on the abdomen and the lower esophageal sphincter.
Alternative medicine
Some complementary and alternative therapies, such as ginger, chamomile and slippery elm, may be recommended to treat GERD. However, none have been proved to treat GERD or reverse damage to the esophagus. Talk to a healthcare professional if you're considering taking alternative therapies to treat GERD.
Preparing for an appointment
You may be referred to a doctor who specializes in the digestive system, called a gastroenterologist.
What you can do
- Be aware of any pre-appointment restrictions, such as restricting your diet before your appointment.
- Write down your symptoms, including any that may seem unrelated to the reason why you scheduled the appointment.
- Write down any triggers to your symptoms, such as specific foods.
- Make a list of all your medicines, vitamins and supplements.
- Write down your key medical information, including other conditions.
- Write down key personal information, along with any recent changes or stressors in your life.
- Write down questions to ask your doctor.
- Ask a relative or friend to go with you, to help you remember what was talked about.
Questions to ask your doctor
- What's the most likely cause of my symptoms?
- What tests do I need? Is there any special preparation for them?
- Is my condition likely temporary or chronic?
- What treatments are available?
- Are there any restrictions I need to follow?
- I have other health concerns. How can I best manage these conditions together?
In addition to the questions that you've prepared, don't hesitate to ask questions during your appointment anytime you don't understand something.
What to expect from your doctor
You're likely to be asked a few questions. Being ready to answer them may leave time to go over points you want to spend more time on. You may be asked:
- When did you begin experiencing symptoms? How severe are they?
- Have your symptoms been continuous or occasional?
- What, if anything, seems to improve or worsen your symptoms?
- Do your symptoms wake you up at night?
- Are your symptoms worse after meals or lying down?
- Does food or sour material ever come up in the back of your throat?
- Do you have trouble swallowing food, or have you had to change your diet to avoid difficulty swallowing?
- Have you gained or lost weight?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use