
Glioblastoma
Conditions
Overview
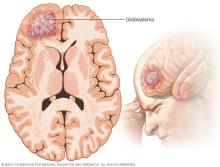
Glioblastoma is an aggressive type of brain cancer that starts in cells called astrocytes, which support nerve cells. Because it begins in these glial cells, glioblastoma is part of a wider group of tumors called gliomas. Glioblastoma is the most common malignant form of glioma. It's the most common malignant brain tumor in adults and makes up about half of all malignant brain tumors in adults.
Within this group, glioblastoma is classified as a grade 4 glioma, the most serious type of glioma. Grade 4 means the tumor grows and spreads quickly into nearby brain tissue, which makes it hard to remove completely. As a result, these tumors can invade and destroy healthy tissue.
Glioblastoma is sometimes called GBM. The older term "glioblastoma multiforme" refers to the same disease.
Glioblastoma can occur at any age, but it happens most often in older adults. Symptoms vary based on where the tumor forms in the brain and may involve seizures or changes in thinking, speech, vision, strength, sensation or balance.
There is no cure for glioblastoma. Treatments such as surgery, radiation and chemotherapy may slow tumor growth, ease symptoms and help people live longer.
Symptoms
Signs and symptoms of glioblastoma can vary based on where the tumor forms in the brain.
Common glioblastoma symptoms include:
Headache and related symptoms:
- Frequent or worsening headaches.
- Headaches that are worse in the morning.
- Headaches that get worse when lying down.
- Nausea or vomiting.
Changes in thinking and memory:
- Confusion or trouble understanding information.
- Difficulty making decisions.
- Memory loss or difficulty concentrating.
Personality and behavior changes:
- Irritability.
- Reduced ability to control emotions.
- Noticeable shifts in behavior or mood.
- Restlessness and agitation.
Sensory symptoms:
- Vision issues such as blurred or double vision or loss of side vision.
- Hearing changes or ringing in the ears.
- Changes in sensation such as numbness or reduced sense of touch.
- Changes in smell or taste.
Speech and language difficulties:
- Difficulty finding words.
- Difficulty understanding language.
- Slurred or unclear speech.
Movement and coordination problems:
- Difficulty with balance or coordination.
- Weakness in the face, arms or legs.
- Weakness that affects one side of the body.
- Difficulty swallowing.
Seizures and changes in alertness:
- New seizures in someone without a prior seizure history.
- Increased tiredness or sleepiness.
- Brief periods of being less alert or harder to wake.
When to see a doctor
Make an appointment with a doctor or other healthcare professional if you have any signs or symptoms that worry you.
Causes
The cause of most glioblastomas is not known.
Glioblastoma happens when cells in the brain develop changes in their DNA. Healthcare professionals sometimes call these changes mutations or variations. DNA gives cells instructions for how to grow, divide and die.
When DNA changes occur, the instructions change. The cells may grow too fast, make too many copies or keep living when healthy cells would die. These changed cells become cancer cells.
The cancer cells can build up and form a tumor. As the tumor grows, it can press on nearby nerves and parts of the brain. It also can invade and destroy healthy brain tissue, leading to symptoms and complications.
Most glioblastomas do not run in families, and inherited causes are rare.
Risk factors
Researchers do not know why most glioblastomas develop, but a few factors have been linked to a higher risk. Factors that can increase the risk of glioblastoma include:
- Getting older. Glioblastoma is most common in older adults. But it can happen at any age.
- Being exposed to radiation. People who have been exposed to a type of radiation called ionizing radiation have an increased risk of glioblastoma. One example of ionizing radiation is radiation therapy used to treat cancer.
- Inherited syndromes that increase cancer risk. In some families, DNA changes passed from parents to children may increase the risk of glioblastoma. Inherited syndromes may include Lynch syndrome and Li-Fraumeni syndrome. Genetic testing can find these syndromes.
- Being assigned male at birth. Glioblastoma is about 1.5 times more common in people assigned male at birth.
Researchers haven't found anything you can do to prevent glioblastoma.
Complications
Glioblastoma can cause complications as it grows and affects nearby brain tissue. Which complications happen depends on the tumor's size and location. Possible complications include:
- Seizures. Glioblastoma may cause new seizures or make existing seizures worse.
- Brain swelling. Tumor growth can lead to swelling in the brain, which may cause headache, nausea or changes in alertness.
- Changes in thinking or personality. Glioblastoma can affect memory, planning, attention or behavior.
- Weakness or changes in movement. Tumors in certain areas can cause weakness on one side of the body or make coordination difficult.
- Trouble with vision or speech. Glioblastoma may affect how someone sees or speaks depending on where it forms.
- Hydrocephalus. In some cases, the tumor blocks the flow of fluid around the brain, causing a buildup of pressure.
- Glioblastoma that comes back. Even with treatment, glioblastoma often returns. When this happens, symptoms may become more noticeable and additional treatment may be needed.
Prevention
There is no known way to prevent glioblastoma. Most glioblastomas happen without a clear cause, and researchers have not found any lifestyle changes that lower the risk.
Avoiding unnecessary exposure to ionizing radiation may reduce risk, but this type of radiation is not common in daily life.
Diagnosis
To diagnose glioblastoma, you may have a physical exam and a review of your personal and medical history. You also may have tests to check how your brain is working and to take pictures of your brain.
Tests and procedures used to diagnose glioblastoma include:
- Neurological exam. This type of exam checks vision, hearing, balance, coordination, strength and reflexes. Changes in one or more of these areas might give clues about the part of the brain the glioblastoma affects.
- Imaging tests. Imaging tests can help find the location and size of a glioblastoma. A brain MRI is the imaging test used most often to diagnose glioblastoma. Sometimes, you have an IV injection of contrast material before your MRI. This helps create better pictures. Other imaging tests may include brain CT and positron emission tomography, which also is called a PET scan.
-
Biopsy. A biopsy is a procedure to remove a sample of tissue for testing. It can be done with a needle before surgery or during surgery to remove the glioblastoma. The sample is sent to a lab for testing. Tests can tell whether the cells are cancerous and whether they're glioblastoma cells.
Special tests of the cancer cells can give your healthcare team more information about your glioblastoma and your prognosis. The team uses this information to create a treatment plan.
Treatment
There are several kinds of cancer therapy that may be used to treat glioblastoma. Glioblastoma treatment may begin with surgery if the tumor can be safely accessed. But surgery isn't always an option. For example, if the glioblastoma grows deeper into the brain, it might be too risky to remove much of the cancer. If that happens, only a biopsy may be considered. Other treatments, such as radiation therapy and chemotherapy, might be recommended as the first treatment.
The treatments that are right for you depend on your particular situation. Your healthcare team considers the size of the glioblastoma and where it's located in the brain. Your treatment plan also depends on your health and your preferences.
Glioblastoma treatment options include:
Surgery to remove the glioblastoma
A brain surgeon, also called a neurosurgeon, works to remove as much of the glioblastoma as can be done safely. There are different types of brain tumor surgery that may be used to remove a glioblastoma. Glioblastoma often grows into nearby brain tissue, so it is not expected that surgery can remove all of the cancer cells. Most people have other treatments after surgery to kill the cancer cells that are left.
Radiation therapy
Radiation therapy treats cancer with powerful energy beams called radiation. The energy can come from sources such as X-rays and protons. During radiation therapy, you lie on a table while a machine moves around you. The machine aims the radiation at specific areas in your brain.
Radiation therapy is usually recommended after surgery to kill any remaining cancer cells. It might be combined with chemotherapy. For people who can't have surgery, radiation therapy and chemotherapy may be the main treatments.
Chemotherapy
Chemotherapy treats cancer with strong medicines. A chemotherapy medicine taken as a pill is often used after surgery and during and after radiation therapy. Other types of chemotherapy given through a vein may be used for glioblastoma that returns.
Sometimes thin, circular wafers containing chemotherapy medicine might be put in the brain during surgery. The wafers dissolve slowly, releasing the medicine to kill cancer cells.
Tumor treating fields therapy
Tumor treating fields therapy (TTF) is a treatment that uses electrical energy to damage glioblastoma cells. TTF makes it hard for the cells to multiply.
During this treatment, sticky pads are attached to the scalp. You might need to shave your head so that the pads can stick. Wires connect the pads to a portable device. The device generates an electrical field that interrupts the signals glioblastoma cells need to divide.
TTF works with chemotherapy. It might be suggested after radiation therapy.
Targeted therapy
Targeted therapy uses medicines that attack unique biomarkers in the cancer cells. By blocking these biomarkers, targeted treatments can cause cancer cells to die.
One targeted medicine used for some people with glioblastoma is bevacizumab (Avastin). It does not cure glioblastoma, but it may help shrink the tumor or reduce swelling and symptoms in some people, especially when the cancer comes back after treatment.
Your glioblastoma cells may be tested to see if targeted therapy might help you. Targeted therapy is sometimes used after surgery if the glioblastoma can't be removed completely. Targeted therapy also may be used for glioblastoma that comes back after treatment.
Clinical trials
Researchers are studying many promising treatments for glioblastoma. Trials may look at new medicines, new combinations of treatments or new ways of delivering treatment. Some trials are testing approaches such as immunotherapy, vaccines or cell-based therapies. These treatments are not part of standard care, but they may offer options for some people.
Clinical trials are studies of new treatments that may not yet be proved to be effective. These studies provide a chance to try the latest treatments that have the potential to help. The risk of side effects might not be known.
Treatments such as chimeric antigen receptor (CAR)-T cell therapy are being studied in clinical trials for glioblastoma but are not part of standard treatment. CAR T-cell therapy is a type of immunotherapy that changes a person's own immune cells so they can better recognize and attack cancer. Researchers are studying whether this approach could help treat glioblastoma, but it is only available in clinical trials at this time.
Treatments to control symptoms
If your glioblastoma is causing symptoms, you might need medicine to help you feel more comfortable. Which medicines you need depends on your situation. Options might include:
- Medicine to control seizures.
- Steroid medicines to reduce brain swelling.
- Medicine to help with headaches.
Palliative care
Palliative care is a special type of healthcare that helps someone with a serious illness feel better. If you have cancer, palliative care can help relieve pain and other symptoms. Palliative care does not try to cure the cancer. A healthcare team that may include doctors, nurses and other specially trained health professionals provides palliative care. The care team's goal is to improve quality of life for you and your family.
Palliative care specialists work with you, your family and your care team. They provide an extra layer of support while you have cancer treatment. You can have palliative care at the same time you're getting strong cancer treatments, such as surgery, chemotherapy or radiation therapy.
The use of palliative care with other medical treatments can help people with cancer feel better and live longer.
Alternative medicine
Alternative medicine therapies can't cure glioblastoma. But some integrative treatments can be combined with your healthcare team's care to help you cope with cancer treatment and side effects, such as distress.
People with cancer often feel distress. If you're distressed, you may have difficulty sleeping and find that you are thinking about your cancer all the time.
Discuss your feelings with your healthcare team. Specialists can help you come up with strategies for coping. For some people, medicines may help.
Integrative medicine treatments that may help you feel better include:
- Art therapy.
- Exercise.
- Massage therapy.
- Meditation.
- Music therapy.
- Relaxation exercises.
- Spirituality.
Talk with your healthcare team if you're interested in these treatment options.
Coping and support
With time, you'll find what helps you cope with the uncertainty and worry of a cancer diagnosis. Until then, you may find it helps to:
Learn enough about glioblastoma to make decisions about your care
Ask your healthcare team about your cancer, including your test results, treatment options and, if you like, your prognosis. As you learn more about glioblastoma, you may become more confident in making treatment decisions.
Keep friends and family close
Keeping your close relationships strong can help you deal with glioblastoma. Friends and family can provide the practical support you may need, such as helping take care of your home if you're in the hospital. And they can serve as emotional support when you feel overwhelmed by having cancer.
Find someone to talk with
Find someone who is willing to listen to you talk about your hopes and worries. This may be a friend or family member. The concern and understanding of a counselor, medical social worker, clergy member or cancer support group also may be helpful.
Ask your healthcare team about support groups in your area. Other sources of information include the National Cancer Institute and the American Cancer Society. Some support groups and online communities focus specifically on brain tumors or glioblastoma.
Preparing for an appointment
Make an appointment with a doctor or other healthcare professional if you have any symptoms that worry you.
If your healthcare professional thinks you might have a brain tumor, such as glioblastoma, you may be referred to a specialist. Specialists who care for people with glioblastoma include:
- Doctors who specialize in brain nervous system diseases, called neurologists.
- Doctors who use medicine to treat cancer, called medical oncologists.
- Doctors who use radiation to treat cancer, called radiation oncologists.
- Doctors who specialize in brain and nervous system cancers, called neuro-oncologists.
- Surgeons who operate on the brain and nervous system, called neurosurgeons.
Because appointments can be brief, it's a good idea to be prepared. Here's some information to help you get ready.
What you can do
- Be aware of anything you need to do ahead of time. When you make the appointment, be sure to ask whether there's anything you need to do in advance, such as restrict your diet.
- Write down symptoms you have, including any that may not seem related to the reason for the appointment.
- Write down important personal information, including major stresses or recent life changes.
- Make a list of all medicines, vitamins and supplements you're taking and the doses.
- Take a family member or friend along. Sometimes it can be very hard to remember all the information you get during an appointment. Someone who goes with you may remember something that you missed or forgot.
- Write down questions to ask your healthcare team.
Your time with your healthcare team is limited, so preparing a list of questions can help you make the most of your time together. List your questions from most important to least important in case time runs out. For glioblastoma, some basic questions to ask include:
- In what part of the brain is my cancer located?
- Has my cancer spread to other parts of my body?
- Will I need more tests?
- What are the treatment options?
- How much does each treatment increase my chances of living longer?
- What are the possible side effects of each treatment?
- How will each treatment affect my daily life?
- Is there one treatment option you believe is the best?
- What would you recommend to a friend or family member in my situation?
- Should I see a specialist?
- Are there any brochures or other printed material that I can take with me? What websites do you recommend?
- What will determine whether I should plan for a follow-up visit?
Don't hesitate to ask other questions.
What to expect from your doctor
Be prepared to answer questions, such as:
- When did you first begin having symptoms?
- Do you always have symptoms or do they come and go?
- How bad are your symptoms?
- What, if anything, seems to make your symptoms better?
- What, if anything, seems to worsen your symptoms?
Survival rates
Survival rates describe how groups of people with glioblastoma have done over time. These numbers cannot predict exactly what will happen for you, but they can give a general sense of how this cancer behaves and how age and treatment may affect outlook.
5-year and 10-year survival rates for glioblastoma
Glioblastoma is a fast-growing brain cancer. Even with treatment, long-term survival is uncommon. In large studies, about 5% to 7% of people are alive five years after diagnosis.
Some people live longer, but 10-year survival is rare. Long-term survivors do exist, and their experiences can vary widely.
Survival rates cannot predict exactly what will happen for any one person. They give a general picture of how this cancer behaves when looking at many people over time.
Glioblastoma survival rates by age
Age is one of the strongest factors affecting life expectancy in glioblastoma. Younger adults often respond better to treatment and may live longer.
In general:
- Younger adults tend to have a better outlook. People younger than 45 years old at the time of diagnosis make up a larger share of long-term survivors.
- Middle-aged adults often have a life expectancy close to the overall average of 12 to 18 months.
- Older adults, especially those over 65 to 70, may live a shorter time because glioblastoma grows quickly and some treatments may be harder to tolerate.
Glioblastoma in children is rare. When it does occur, some children live longer than adults, especially if surgery and other treatments can be done safely.
What affects prognosis and life expectancy in glioblastoma
Many factors can influence life expectancy for someone with glioblastoma. These factors can affect how well treatment works and how the tumor behaves over time.
Factors include:
- Age. Younger adults often respond better to treatment.
- Overall health. People who are active and independent at diagnosis may tolerate treatment better.
- Tumor location. Tumors in certain areas of the brain may limit how much treatment is safe to give.
- Surgery. Removing more of the tumor, when it is safe to do so, is linked with longer survival.
- Tumor features. Certain biomarker lab tests, such as MGMT promoter methylation, can show how well the tumor may respond to treatment.
Your healthcare team can explain how these factors apply to your situation.
What are the different grades of glioma and what does grade 4 mean?
Brain and spinal cord tumors are grouped into grades based on how the cells look under a microscope and how quickly they are likely to grow. The World Health Organization (WHO) uses grades from 1 to 4.
- Grade 1 and 2 gliomas tend to grow slowly.
- Grade 3 gliomas grow faster and can spread into nearby brain tissue.
- Grade 4 gliomas grow the fastest and are the most invasive into nearby brain tissue.
Glioblastoma is by definition a grade 4 diffuse glioma. There is no such thing as a "low-grade" or grade 1, 2 or 3 glioblastoma.
Glioblastomas are a type of glioma called IDH-wildtype glioma. Some tumors that used to be called IDH-mutant glioblastoma have been renamed and are now termed grade 4 astrocytomas, which is a separate type of glioma. You also may hear terms such as butterfly glioblastoma, which describes how the tumor looks on imaging. This term does not describe a separate type of tumor.
Is there a difference between malignant and nonmalignant glioblastoma?
All glioblastomas are considered malignant brain tumors. The term "nonmalignant glioblastoma" is not used in medicine.
Some brain tumors are called benign or nonmalignant, such as certain low-grade astrocytomas or meningiomas. These tumors are not cancerous, grow more slowly and usually have a much better outlook than glioblastoma does.
If you see the term "malignant glioblastoma," it is simply emphasizing that glioblastoma is a fast-growing cancer. It is not describing a separate type of tumor.
Changes that may happen as glioblastoma advances
As glioblastoma grows or returns after treatment, symptoms may become more noticeable. These changes happen at different times for different people. The changes can include:
- More tiredness or sleeping more.
- Trouble thinking clearly or remembering things.
- More weakness or changes in balance.
- More trouble with speech or understanding language.
- More-frequent or harder-to-control seizures.
- Changes in eating or swallowing.
- Less awareness of what is happening.
These changes often happen gradually as glioblastoma advances and may be more noticeable in the final months or weeks of life.
Prognosis
Learning about the prognosis for glioblastoma can feel overwhelming. Prognosis describes what healthcare teams know about how the cancer may behave over time. Everyone's experience is different, but research can give a general idea of life expectancy and the factors that may affect it.
What is the life expectancy for someone with glioblastoma?
Glioblastoma is an aggressive form of brain cancer, and life expectancy can vary widely from person to person. Many factors influence life expectancy, including:
- Your age.
- Your overall health.
- Where the glioblastoma is in the brain.
- How much of the tumor can be safely removed with surgery.
- How well the glioblastoma responds to treatment.
In large studies, people with glioblastoma have a median life expectancy of about 12 to 18 months after diagnosis when they receive standard treatment. Standard treatment typically includes surgery when possible, followed by radiation therapy and chemotherapy. Some people live longer if they can complete the full treatment plan and if their tumor responds well to treatment.
How treatment affects life expectancy for glioblastoma
Treatments such as surgery, radiation therapy and chemotherapy do not cure glioblastoma, but they can help people live longer and reduce symptoms so they can live more comfortably. Some people also receive tumor treating fields therapy or take part in clinical trials.
Without treatment, glioblastoma usually grows quickly. In these situations, people may live only a few months.
Treatment can:
- Slow how fast the tumor grows.
- Reduce symptoms such as headaches, seizures or weakness.
- Help people stay independent for longer.
Your healthcare team can explain the treatment options that match your situation and how each option may affect your outlook.
Life expectancy after glioblastoma recurrence
Even with treatment, glioblastoma almost always comes back after the first treatment. This is called recurrence or progression.
When glioblastoma returns, life expectancy is usually shorter than it was at the first diagnosis. In many studies, people live about 6 to 12 months after the tumor begins to grow again, though this varies from person to person.
How long someone lives after recurrence depends on:
- Their age and overall health.
- Where the tumor is located.
- How quickly the tumor is growing.
- What treatments they can receive after recurrence, such as surgery, chemotherapy, targeted therapy, tumor treating fields therapy or clinical trials.
Some people may live longer if they can have additional treatment. Others may choose palliative care that focuses on comfort.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use