
Hip dysplasia
Conditions
Overview
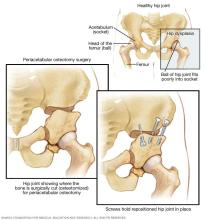
Hip dysplasia is the medical term for a hip socket that doesn't fully cover the ball portion of the upper thighbone. This allows the hip joint to become partially or completely dislocated. Most people with hip dysplasia are born with the condition.
Healthcare professionals will check your baby for signs of hip dysplasia shortly after birth and during well-baby visits. If hip dysplasia is diagnosed in early infancy, a soft brace can usually correct the problem.
Mild hip dysplasia might not start causing symptoms until a person is a teenager or young adult. Hip dysplasia can damage the cartilage lining the joint. It also can hurt the soft cartilage, called the labrum, that rims the socket portion of the hip joint. This is called a hip labral tear.
In older children and young adults, surgery may be needed to move the bones into the proper positions for smooth joint movement.
Symptoms
Symptoms vary by age group. In infants, you might notice that one leg is longer than the other. Once a child begins walking, a limp may develop. During diaper changes, one hip may be less flexible than the other.
In teenagers and young adults, hip dysplasia can cause painful complications such as osteoarthritis or a hip labral tear. This may cause activity-related groin pain. Sometimes, there might be a sensation of instability in the hip.
Causes
At birth, the hip joint is made of soft cartilage that gradually hardens into bone. The ball and socket need to fit together well because they act as molds for each other. If the ball isn't seated firmly into the socket, the socket will not fully form around the ball and will become too shallow.
During the final month before birth, the space within the womb can become so crowded that the ball of the hip joint moves out of its proper position. This results in a shallower socket. Factors that may reduce the amount of space in the womb include:
- First pregnancy.
- Large baby.
- Breech presentation.
Risk factors
Hip dysplasia tends to run in families and is more common in girls. The risk of hip dysplasia is also higher in babies born in the breech position and in babies who are swaddled tightly with the hips and knees straight.
Complications
Later in life, hip dysplasia can damage the soft cartilage, called the labrum, that rims the socket portion of the hip joint. This is called a hip labral tear. Hip dysplasia can also make the joint more likely to develop osteoarthritis. This happens because of higher contact pressures over a smaller surface of the socket. Over time, this wears away the smooth cartilage on the bones that helps them glide against each other as the joint moves.
Diagnosis
During well-baby visits, healthcare professionals typically check for hip dysplasia by moving an infant's legs into a variety of positions that help indicate whether the hip joint fits together well. If hip dysplasia is suspected, a hip ultrasound might be ordered to check the hip joint for signs of dysplasia.
Mild cases of hip dysplasia can be difficult to diagnose and might not start causing problems until you're a young adult. If your healthcare team suspects hip dysplasia, they might suggest imaging tests, such as X-rays or magnetic resonance imaging (MRI).
Treatment
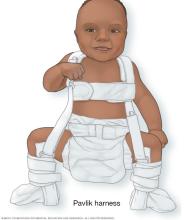

Hip dysplasia treatment depends on the age of the affected person and the extent of the hip damage. Infants are usually treated with a soft brace, such as a Pavlik harness, that holds the ball portion of the joint firmly in its socket for several months. This helps the socket mold to the shape of the ball.
The brace doesn't work as well for babies older than 6 months. Instead, the healthcare professional may move the bones into the proper position and then hold them there for several months with a full-body cast. Sometimes surgery is needed to fit the joint together properly.
If the dysplasia is more serious, the position of the hip socket also can be corrected. In a periacetabular (per-e-as-uh-TAB-yoo-lur) osteotomy, the socket is repositioned in the pelvis so that it matches up better with the ball.
Hip replacement surgery might be an option for older people whose dysplasia has severely damaged their hips over time, resulting in debilitating arthritis.
Preparing for an appointment
You'll probably first bring your concerns to your family healthcare professional. They might refer you to an orthopedic surgeon.
What you can do
Before your appointment, you might want to:
- Write down any signs and symptoms you or your child are experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Make a list of any medicines, vitamins or supplements that you or your child are taking.
- Consider taking a family member or friend along. Sometimes it can be difficult to remember all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Request that a copy of previous medical records be forwarded to your current healthcare professional, if you're changing care teams.
- Write down questions to ask the healthcare team.
Your time with the healthcare professional is limited, so preparing a list of questions can help you make the most of your time together. Some basic questions to ask include:
- What's the most likely cause of the symptoms?
- What kinds of tests are needed? Do these tests require any special preparation?
- What treatments are available, and which do you recommend?
- What are the possible side effects from treatment?
- Are there any brochures or other printed material that I can take home with me?
- Can you recommend any websites for more information on hip dysplasia?
In addition to the questions that you've prepared to ask your healthcare team, don't hesitate to ask questions during your appointment at any time if you don't understand something.
What to expect from your doctor
Your healthcare professional is likely to ask you a number of questions. Being ready to answer them may reserve time to go over any points you want to spend more time on. Your doctor may ask:
- When did you or your child first begin experiencing symptoms?
- Have the symptoms been continuous or occasional?
- Does anything seem to improve the symptoms?
- What, if anything, appears to worsen the symptoms?
- If you or your child has already been diagnosed with hip dysplasia, when and where was the diagnosis made?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use