
Nerve sheath tumors
Conditions
Overview
Nerve sheath tumors are the most common type of peripheral nerve tumor. Peripheral nerve tumors are growths that develop in or around nerves that connect the brain and spinal cord to the rest of the body. Depending on the nerve involved, these tumors can affect movement, sensation or both.
Nerve sheath tumors form in the protective covering around nerves and can develop along any peripheral nerve in the body. They may occur in the arms or legs, along spinal nerve roots, or on the cranial nerves that control hearing, balance and facial movement.
Most nerve sheath tumors are benign and tend to grow slowly. But they can press on nearby nerves or tissues and lead to pain, numbness, tingling or loss of function. A small number of these tumors are malignant and can grow quickly or spread to other parts of the body.
Nerve sheath tumors may be found during imaging for another reason or after symptoms begin. Many can be monitored with imaging or removed with surgery. When surgery risks harming nearby nerves, you may have other treatments.
Because most nerve sheath tumors are benign, staging is not needed. Malignant tumors can grow faster, invade nearby tissues, or spread. These tumors may require staging and a broader treatment approach. Prognosis depends on the type of tumor, how fast it grows, and whether it can be removed safely.
Types
Nerve sheath tumors are a type of peripheral nerve tumor. They include several benign tumor types and a smaller number of malignant tumor types.
Schwannomas (benign)
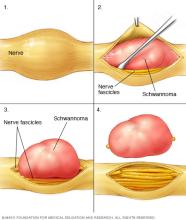
Schwannomas are the most common nerve sheath tumors. They usually grow slowly and form a clear border that pushes nerve fibers aside rather than growing through them. Schwannomas can occur along spinal nerve roots or cranial nerves involved in hearing and balance.
Vestibular schwannomas (benign)
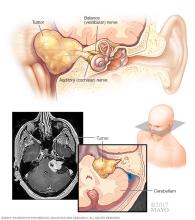
A vestibular schwannoma, previously called an acoustic neuroma, is a schwannoma that forms on the vestibulocochlear nerve. This nerve controls hearing and balance. These tumors grow along the internal auditory canal at the skull base. They are therefore classified as a type of skull base tumor. As a vestibular schwannoma grows, it may affect hearing, balance or nearby cranial nerves. It is a type of nerve sheath tumor.
Neurofibromas (benign)
Neurofibromas grow within the nerve and mingle with the nerve fibers.
Plexiform neurofibromas (usually benign)
Plexiform neurofibromas involve multiple branches of a nerve. They can extend through nearby soft tissues. Depending on their size and location, they may change how the affected body part moves or feels. These tumors occur most often in people with neurofibromatosis type 1. Most plexiform neurofibromas are benign, but certain types can get larger over time and have a risk of becoming malignant.
Hybrid nerve sheath tumors (usually benign)
Hybrid tumors have features of more than one benign tumor type, most often schwannoma and neurofibroma. They tend to behave like benign tumors but can appear in people with genetic syndromes that cause multiple nerve tumors.
Spinal nerve root tumors (benign)
Spinal nerve root tumors are nerve sheath tumors that begin on or near the nerves exiting the spinal cord. Schwannomas and neurofibromas commonly arise from spinal nerve roots and may grow inside or outside the covering around the spinal cord. These tumors can cause back pain, limb symptoms or signs of pressure on the spinal cord. Nerve root involvement means the tumor is growing on or pressing against a spinal nerve root. This can affect movement or sensation in the areas served by that nerve.
Cranial nerve tumors (benign)
Cranial nerves can develop nerve sheath tumors, most often schwannomas. These tumors can form along several cranial nerves. These include the nerve for facial sensation, also called the trigeminal nerve, the nerve that controls swallowing and voice, also called the vagus nerve, and nerves for hearing and balance. Tumors in these locations may affect hearing, facial movement, swallowing or speech depending on their size and where they grow.
Malignant peripheral nerve sheath tumors
Malignant peripheral nerve sheath tumors (MPNSTs) are rare cancerous tumors that can grow quickly or spread. They may arise on their own or develop from a plexiform neurofibroma. MPNSTs occur most often in people with neurofibromatosis type 1. They also tend to grow in areas previously treated with radiation. A nerve tumor is considered a sarcoma when it becomes malignant and grows into nearby tissue or spreads to other areas of the body.
Which nerves can develop sheath tumors?
Any peripheral nerve can develop a sheath tumor. These tumors may appear along:
- Major nerves in the chest or arms, including the brachial plexus.
- Major nerves in the legs, including the sciatic nerve.
- Spinal nerve roots.
- Cranial nerves such as the vestibulocochlear, trigeminal and vagus nerves.
Are brain tumors the same as nerve sheath tumors?
Brain tumors and nerve sheath tumors are not the same. Brain tumors form from cells within the brain. Nerve sheath tumors start on peripheral nerves or cranial nerves but not in brain tissue.
Symptoms
The symptoms of a nerve sheath tumor develop from direct effects on the main nerve or from the tumor pressing on nearby nerves, blood vessels or tissues. As the tumor grows, it may be more likely to cause symptoms, although tumor size doesn't always determine effects.
Because nerve sheath tumors can form anywhere along the nerves, symptoms vary by location and the structures involved. Some tumors cause no symptoms at all. A larger tumor may be more likely to cause symptoms, although size alone does not predict how someone will feel.
Skin or surface changes
You may notice skin or surface changes on or near the tumor site. These changes can reflect a slow-growing lump along a peripheral or spinal nerve. They may be sensitive when touched. You may have:
- A lump or swelling under the skin.
- A tender area that is sore when pressed.
- A feeling of fullness or pressure in the area.
Sensory changes
These symptoms affect how an area feels. They may occur when a tumor irritates or compresses sensory fibers, a sensory nerve or a nerve root. This leads to changed or increased sensation. Symptoms include:
- Tingling or numbness.
- Burning or shocklike sensations.
- Heightened sensitivity to touch.
Changes in strength or movement
These symptoms relate to how muscles work. They may appear when a nerve sheath tumor affects a motor branch or compresses the spinal cord or nerve root. This can limit signals that support movement. You may feel:
- Weakness in the affected area.
- Reduced ability to move the area.
- Muscle cramping or shrinking over time.
Symptoms linked to specific nerve locations
Some symptoms appear when tumors affect cranial or spinal nerves. These symptoms may reflect pressure on hearing or balance pathways, facial nerve involvement, or irritation of spinal roots that send signals into the arms or legs. You may feel:
- Dizziness or changes in balance.
- Hearing changes, such as ringing or reduced hearing.
- Changes in facial movement.
- Back or neck discomfort or pain that travels into an arm or a leg.
When to see a doctor
See your healthcare professional if you have any of the symptoms listed, especially if you have a lump that grows quickly.
Causes
It's not clear why most nerve sheath tumors develop. These tumors develop from the cells that surround and support peripheral nerves, spinal nerve roots or cranial nerves.
Inherited conditions
Some nerve sheath tumors are linked to inherited conditions that affect how nerve cells grow. Inherited means a gene change is present at birth and can be passed down in families. Neurofibromatosis type 1 (NF1) increases the risk of having neurofibromas, plexiform neurofibromas and malignant peripheral nerve sheath tumors.
Neurofibromatosis type 2 and schwannomatosis are linked to having multiple schwannomas along spinal nerve roots or cranial nerves. These conditions are caused by changes in genes such as NF1, NF2, SMARCB1 and LZTR1. These genes help guide cell growth.
Genetic changes that are not inherited
For many people, the cause of a nerve sheath tumor is not known. Most tumors appear after genetic changes develop within the cells of the nerve sheath. These changes can affect how the cells control their growth. These changes often happen randomly and are not inherited.
How nerve sheath tumors begin
Nerve sheath tumors form when Schwann cells or other cells around the nerve grow in a way that is not controlled. These cells usually help protect and insulate nerves, but genetic changes can cause them to form a lump of extra cells that grow in one area rather than spreading throughout the nerve.
How some tumors can turn into cancer
Malignant peripheral nerve sheath tumors often develop from long-standing plexiform neurofibromas, especially in people with neurofibromatosis type 1. These malignant tumors are linked to other genetic changes that allow cells to grow quickly or invade nearby tissues. Only a small number of benign nerve sheath tumors become cancerous.
Less common causes
Prior radiation exposure is a less common cause. Radiation therapy can lead to genetic changes in nerve sheath cells years after treatment. It also may increase the risk of developing a benign nerve sheath tumor or malignant peripheral nerve sheath tumor.
What does not cause nerve sheath tumors
Most nerve sheath tumors are not caused by injury. An injury may draw attention to a tumor that is already present, but injuries do not cause tumors to form.
Risk factors
Nerve sheath tumors most often develop from the cells that support and surround nerves. Factors that affect how these cells grow, repair damage or form supportive tissue can increase the chance of developing a tumor.
Some people develop nerve sheath tumors with no known risk factors. These tumors can develop in anyone, but certain conditions or exposures can make them more likely. These factors influence how nerve cells grow, repair damage or form supportive tissue around nerves.
Having a risk factor does not predict how many tumors will form or how they will behave. The lack of risk factors does not eliminate the possibility of having a tumor.
Genetic conditions
Some conditions change how nerve cells develop and significantly increase the chance of having one or more nerve sheath tumors. These include:
- Neurofibromatosis type 1 (NF1).
- NF2-related schwannomatosis.
- Other forms of schwannomatosis.
These conditions are inherited, meaning that they can run in families. As a result, tumors can form along nerves throughout the body, and some people have many tumors over time. Most of these tumors are benign, but their number and location can influence symptoms.
History of radiation exposure
Exposure to radiation, especially earlier in life, can increase the chance of having a nerve sheath tumor years later. This is most often linked to previous radiation used to treat another condition. Even so, radiation-related nerve sheath tumors are uncommon.
Complications
Some complications of nerve sheath tumors may be lasting if a nerve is compressed or affected for a long time.
Nerve sheath tumors can interfere with how nerves work by putting pressure on the nerves from which they grow, on nearby nerves or on the spinal cord. If this pressure continues, some changes may not fully improve even after treatment. The type of complication depends on where the tumor forms and how long the nerve has been affected.
Long-term weakness or loss of movement
Persistent pressure on a nerve can limit its ability to send signals to the muscles it serves. Over time this may lead to lasting weakness or reduced function of the affected area.
Lasting changes in feeling
If a nerve has been pressed on for a long time, feeling in that area or function of the nerve may not completely return.
Changes in how the area works
Depending on the nerve involved, a tumor can make it hard to do tasks such as grasping objects, lifting the foot while walking or coordinating hand movements. Some of these changes can continue even after the tumor is taken out.
Chronic pain
Long-term pain can occur if the nerve has been squeezed, stretched or injured, either from the tumor itself or from treatment.
Changes in balance or coordination
Tumors involving spinal nerve roots or cranial nerves may disrupt pathways that support balance or coordination. Sometimes these changes can become long lasting.
Changes in hearing or facial movement
Tumors on cranial nerves, such as vestibular schwannomas, can lead to lasting hearing loss or weakness of facial muscles if the nerve has been affected for a long time.
Pressure on the spinal cord
Larger tumors in the spine can narrow the space around the spinal cord. If severe, this narrowing can lead to long-term weakness, changes in walking, or loss of bladder or bowel function.
Complications related to malignant tumors
Malignant peripheral nerve sheath tumors are more likely to invade nearby tissues or spread. They can be harder to remove completely and may cause lasting changes in how the affected area moves or feels.
Complications from treatment
Even with careful planning, surgery or radiation may affect how well the nerve works afterward. Some people may have lasting weakness, less sensation or changes in how the nerve works after treatment.
Prevention
There is no known way to prevent most nerve sheath tumors. Many develop without a clear cause. You can't avoid or change the factors that increase risk — such as inherited conditions or prior radiation exposure.
What cannot be prevented
Most nerve sheath tumors occur randomly and are not linked to anything you do or do not do. Conditions such as NF1, NF2-related schwannomatosis and other forms of schwannomatosis are present from birth and cannot be prevented.
What may reduce preventable risk
Although prevention is limited, a few steps can help lower avoidable exposures or support earlier recognition of concerning changes.
- Avoid unnecessary exposure to radiation when alternative options are available.
- Use protective measures during medically necessary radiation, especially in childhood.
- Share any personal or family history of NF1, NF2, or schwannomatosis with members of your care team so they are aware of your risk.
- Have regular care if you have a genetic condition linked to tumor development so your care team can find new growths early.
Understanding limits of prevention
Prevention focuses mainly on reducing avoidable exposures and recognizing tumors early so they can be managed before causing significant symptoms.
Diagnosis
To diagnose a nerve sheath tumor, your care team reviews your health history and asks about any changes you've noticed. These tumors begin in the protective covering around the nerve, called the nerve sheath, so diagnosis focuses on showing whether a growth is coming from this layer. A physical exam and a neurological exam help show how the affected area is working. Several tests can help find out whether a growth arises from the nerve and how it is behaving:
-
Magnetic resonance imaging (MRI). MRI is the primary imaging test for nerve sheath tumors. It provides the clearest view of the nerve and the growth. It is often the first test you have when a nerve tumor is suspected.
This scan uses a magnet and radio waves to create a detailed 3D view of nerves and surrounding tissue. MRI is especially helpful because it can show whether a growth arises from a nerve itself. Many nerve sheath tumors appear as smooth, well-defined masses that follow the path of a nerve. MRI can sometimes show whether a tumor is likely benign or has features that need closer review.
- Computerized tomography (CT). A CT scanner rotates around the body to capture many images. A computer combines them to show a detailed view of the growth and the structures around it.
-
Electromyography (EMG) and nerve ultrasound. These tests are commonly used together to assess nerve health. EMG shows how well a nerve sends signals to muscles. Nerve ultrasound shows the nerve's structure. Together, these tests help pinpoint the affected nerve and clarify how structural changes relate to symptoms.
Small, thin needles are placed into muscles. An instrument records electrical activity as the muscles move, which helps show whether a nerve is sending signals effectively.
Nerve ultrasound uses sound waves to look at nerves just under the skin. The test can show nerve thickening, changes in shape or areas where a tumor may be affecting a nerve. Ultrasound also can help guide further testing or procedures in some situations.
- Nerve conduction study. Often done with an EMG, this test measures how quickly a nerve carries electrical signals to a muscle. It helps show whether a growth is slowing or blocking nerve signals.
- Tumor biopsy. A small sample of the growth is removed and examined under a microscope. Depending on its size and location, the area may be numbed or you may receive medicine that helps you sleep through the procedure. Not every nerve sheath tumor needs a biopsy. Your care team considers biopsy when imaging cannot clearly show whether the tumor is benign or cancerous. Biopsy also is done when the result would change treatment decisions.
-
Nerve biopsy. In some situations, such as when a nerve keeps getting weaker or looks enlarged on imaging, a small piece of the nerve may be removed to help confirm the diagnosis.
Imaging also helps distinguish nerve sheath tumors from other soft tissue growths, such as lipomas or cysts, which often look different on scans.
Because experience matters when interpreting these tests and choosing the safest evaluation approach, many people benefit from working with a care team that frequently diagnoses nerve sheath tumors. Seeking a second opinion can be helpful if you want more information.
Tumor grade
Not every nerve sheath tumor is assigned a numeric grade. Instead, these tumors are placed into broad categories based on how the cells look and how quickly they grow.
A nerve sheath tumor's grade describes how quickly its cells are growing and how different the cells look from nearby tissue when checked in a lab. Grading helps the care team understand how the tumor is likely to behave and which treatment options may be most helpful.
How grading works for nerve sheath tumors
Nerve sheath tumors fall into three categories based on how the cells look under a microscope and how quickly they grow.
- Benign, also called grade 1. Schwannomas and typical neurofibromas grow slowly and look similar to nearby nerve tissue. These tumors are usually managed with monitoring or surgery if they cause symptoms.
- Atypical or intermediate grade. Atypical neurofibromas show early signs of becoming more aggressive. These tumors are watched more closely because some may get worse over time.
- High grade or malignant. Malignant peripheral nerve sheath tumors (MPNSTs) grow quickly, look very different from nearby tissue and can spread. These tumors often need more-intensive treatment because of their aggressive behavior.
Why these tumors don't use grades 1 to 4
Many cancers use a numbered grading system, but nerve sheath tumors generally do not. Benign tumors are consistently grade 1. Tumors with unusual features do not have a standard number grade. Malignant tumors are described as high grade instead of being labeled as grade 3 or grade 4.
These broader categories reflect how these tumors grow and help guide decisions about treatment.
The categories also explain why online searches for terms such as grade 2 schwannoma or grade 4 MPNST often lead to unclear or conflicting results. These labels are not part of current classification systems.
Grading versus staging
Nerve sheath tumors generally do not use a traditional cancer staging system the way many other cancers do. Benign tumors aren't staged. High-grade tumors are mainly described by grade and by whether they have spread.
Treatment
Nerve sheath tumors may be managed with surgery, stereotactic radiosurgery, cancer-directed treatments, rehabilitation or monitoring. The approach depends on the type of tumor, where it is located, and how it affects nerve function.
Surgery
Surgery is used for both benign and malignant tumors depending on size, growth and how the tumor affects nerve function. The goal is to take out the entire tumor while protecting nearby nerves and tissue. When complete removal is not possible, the care team removes as much of the tumor as they safely can.
Surgery is usually considered when the tumor is growing, affects nerve function, causes pain, or has features that raise concern for cancer. Surgery also may be advised when imaging shows that the tumor can be removed safely.
Most nerve sheath tumors are taken out with microsurgery. High-power magnification and nerve-monitoring tools help specialists separate the tumor from the nerve while preserving movement and sensation.
Risks include nerve injury and changes in how the affected area works. These risks depend on the tumor's size and location and the surgical approach. Some tumors can grow back.
Stereotactic radiosurgery
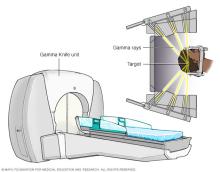
Stereotactic radiosurgery is mainly used for benign tumors located in or around the brain, such as vestibular schwannomas, especially when surgery carries higher risk. Stereotactic radiosurgery also may be considered for some malignant tumors that cannot be removed safely with surgery. It delivers a highly targeted dose of radiation to the tumor without an incision. One form of this treatment is Gamma Knife radiosurgery.
Risks may include weakness or numbness in the treated area or continued tumor growth. Very rarely, radiation exposure may lead to a new tumor in the treated region many years later.
Cancer-directed therapies
These treatments are used only for malignant peripheral nerve sheath tumors, which behave differently from benign tumors and may spread or grow more quickly. Treatment may include surgery, chemotherapy or radiation therapy. The combination used depends on the type of tumor, its location and how it responds to treatment. Cancerous tumors may return after treatment.
Rehabilitation
Rehabilitation is used after treatment for both benign and malignant tumors, especially when surgery or tumor growth affects movement, strength or sensation.
A brace or splint may be used to keep a limb in a position that supports healing. Physical therapists and occupational therapists help rebuild function, improve mobility, and teach strategies that support independence if you've lost a use of a limb or have nerve damage.
Recovery varies based on the tumor's size and location. Many people regain strength and mobility over time. Others may have lasting changes if the nerve was stretched or damaged. Most recovery occurs over weeks to months.
Monitoring and follow-up
Monitoring is an important part of care for many nerve sheath tumors. It helps track changes in tumor size and guides decisions about treatment needs. Monitoring may be used for both benign and malignant tumors, although the timing and goals differ.
Monitoring is most common for benign tumors that are small, slow growing or located in areas where treatment carries higher risk. Monitoring also may be used when the tumor is not affecting movement or sensation.
How often is monitoring needed?
Follow-up typically includes MRI, CT or ultrasound every 6 to 12 months to check for growth or changes in the tumor features. If repeat scans show that the tumor is stable, the timing of imaging may be changed to every few years.
How are malignant nerve sheath tumors monitored?
For malignant nerve sheath tumors, monitoring has different goals. Imaging may be scheduled more often to check for recurrence after treatment. Malignant tumors can return even when they are treated early, so long-term follow-up is advised.
People who have changes in movement, sensation or pain during monitoring should contact their care teams sooner. New symptoms may signal that the tumor is growing or affecting the nerve differently.
Prognosis
Prognosis for malignant nerve sheath tumors varies widely and depends on factors such as tumor size and location and whether the tumor can be removed completely. For all nerve sheath tumors, prognosis also depends on whether the tumor affects nerve function.
Benign tumors often grow slowly and may never cause serious symptoms, especially when they are small or are monitored over time. When benign tumors are removed completely, many do not return.
Some benign tumors can grow back if they cannot be removed fully without harming nearby nerves. In these situations, long-term monitoring helps track changes and guide future treatment.
Malignant nerve sheath tumors tend to grow more quickly and may spread to nearby tissue. Early diagnosis and treatment offer the best chance to control the tumor. Even after treatment, malignant tumors can return, so close follow-up is important.
Prognosis also depends on whether the tumor presses on or grows from a nerve. When nerve fibers are stretched or damaged, changes in movement or sensation may continue even after treatment. Rehabilitation may help improve strength and function over time.
Are benign nerve sheath tumors dangerous?
Most benign nerve sheath tumors grow slowly and may never cause serious symptoms. Many stay stable for years or cause only mild symptoms. Some may grow large enough to press on a nerve or nearby structures, which can affect movement or sensation. These tumors may need treatment to protect nerve function.
Can you live a typical life with a benign nerve sheath tumor?
Yes. Many people live full, active lives with benign nerve sheath tumors, especially when the tumor is small or stable over time. Monitoring helps track changes. Treatment is considered if the tumor begins to affect how the area functions.
Is a nerve sheath tumor a serious condition?
It depends on the tumor type and location. Benign tumors often have an excellent long-term outlook and may not require treatment. Malignant peripheral nerve sheath tumors grow more quickly and may spread, making early diagnosis and treatment important.
Do nerve sheath tumors come back after treatment?
Some benign tumors return if they cannot be removed completely without harming nearby nerves. Malignant tumors have a higher chance of coming back even after treatment. This is why follow-up imaging is important for both benign and malignant tumors.
How does tumor location affect prognosis?
Tumors that grow from or press on major nerves may cause lasting changes in movement or sensation, even if the tumor is treated successfully. Tumors in areas that are hard to access may require careful monitoring or staged treatment.
What is recovery like after nerve tumor removal?
Recovery varies based on tumor size and location. Many people regain strength and movement over time. But others may have lasting changes if the nerve was stretched or damaged. Most recovery occurs over weeks to months.
How fast do nerve sheath tumors grow?
Nerve sheath tumors grow at different rates depending on the tumor type. Many benign tumors grow slowly and may stay stable for years. Plexiform neurofibromas can get larger over time, especially in people with neurofibromatosis type 1. Malignant nerve sheath tumors tend to grow more quickly and may spread.
Can nerve sheath tumors metastasize?
Benign nerve sheath tumors do not metastasize. Only malignant peripheral nerve sheath tumors can metastasize. These tumors can spread to nearby tissue and sometimes to distant sites, which is why early treatment and close follow-up are important.
Coping and support
It can be stressful to deal with the possibility of nerve sheath tumor complications. Making decisions about treatment also can be hard. These suggestions may help:
- Learn as much as you can about nerve sheath tumors. The more you know, the better prepared you'll be to make choices about treatment. Besides talking with your healthcare professional, you may want to talk with a counselor or a social worker. Or you may find it helpful to talk with other people who've had a condition like yours. Ask about their experiences during and after treatment.
- Maintain a strong support system. Family and friends can be a source of support. You may find the concern and understanding of people in a support group to be especially helpful. Your healthcare professional or a social worker may be able to put you in touch with a support group.
Preparing for an appointment
If your primary healthcare professional thinks you have a nerve sheath tumor, you'll likely be referred to a specialist. Specialists include doctors who are experts in conditions of the nervous system, called neurologists, and doctors trained in brain and nervous system surgery, called neurosurgeons.
What you can do
Before the appointment, you might want to prepare a list of answers to the following questions:
- When did you first notice your symptoms?
- Have they gotten worse over time?
- Have your parents or siblings ever had similar symptoms?
- Do you have other medical conditions?
- What medicines or supplements do you take?
- What surgeries have you had?
What to expect from your doctor
Your healthcare professional may ask some of the following questions:
- Do you have pain? If so, where is it?
- Do you have any weakness, numbness or tingling?
- Have your symptoms been constant or do they come and go?
- What treatments have you tried for these symptoms?
Survival rates
Benign nerve sheath tumors usually have a very good long-term outlook. Many stay the same size for years, and others can be removed with surgery. When the entire tumor is taken out, it rarely grows back.
Malignant nerve sheath tumors have a more serious outlook. Outcomes depend on the size of the tumor, how quickly it is growing and whether it can be removed completely. Early diagnosis offers the best chance to control the tumor. These tumors can return even after treatment, so regular follow-up is important.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use