
Pectus excavatum
Conditions
Overview
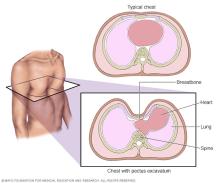
Pectus excavatum is a condition in which the breastbone is sunken into the chest. The sunken breastbone often can be seen shortly after birth. If the breastbone sinks a lot over time, the center of the chest may look like it's been scooped out. This change leaves a deep dent or dip. But many people with the condition just have a slight dip in the breastbone.
This condition also is known as funnel chest. But it can affect much more than the look of the chest. It also can cause symptoms such as shortness of breath, chest pain, and a fast-beating, fluttering or pounding heart. The symptoms tend to become worse during the teenage growth spurt.
The exact cause of pectus excavatum isn't clear. When the condition is serious, it can affect how well the heart and lungs work over time. But even mild pectus excavatum that causes a slight dip in the breastbone can make children feel self-conscious about their bodies.
Surgery to repair pectus excavatum can improve symptoms and the appearance of the chest. But surgery isn't right for everyone with the condition. Other treatment choices may include physical therapy and medical devices.
Symptoms
For many people with pectus excavatum, the only symptom is a slight dip in their chests. In some children, the dip becomes deeper during early puberty. It can keep getting deeper into adulthood.
In people with pectus excavatum, the breastbone may compress the lungs and heart. Symptoms can include:
- A fast-beating, fluttering or pounding heart.
- Chest pain.
- Loss of endurance that becomes worse over time.
- Shortness of breath or extreme tiredness during physical activity.
- A high-pitched whistling sound made while breathing that's triggered by exercise.
- Fainting or dizziness.
- Frequent infections of the upper airway.
- Stress and concern about how the chest looks.
When to see a doctor
See a healthcare professional if you or your child has any symptoms of pectus excavatum. This is key if the symptoms become worse or if the chest keeps becoming more sunken.
Causes
The exact cause of pectus excavatum isn't known. Some experts think it has to do with connective tissue called cartilage. Cartilage that connects the breastbone to the ribs may develop in an irregular way. Genes may play a role in this process.
Risk factors
Pectus excavatum risk factors may include the following:
- Having a family history of pectus excavatum.
- Living with a connective tissue condition such as Marfan syndrome, Ehlers-Danlos syndrome or osteogenesis imperfecta.
- Having a genetic condition such as Noonan syndrome or Turner syndrome.
Complications
Sometimes, pectus excavatum can lead to serious health issues called complications. The complications can affect the heart, lungs and mental health.
Heart and lung trouble
If the depth of the dent in the breastbone is serious, the lungs may not have enough room to fully expand. This also can squeeze the heart. The heart may be pushed to the left and may not pump blood as well as it should. This can cause symptoms such as being less able to exercise, shortness of breath, fast heart rate, and chest pain or pressure.
Self-image concerns
Many people who have pectus excavatum also tend to have a hunched-forward posture. Their lower ribs may flare out and their shoulders may be rounded. Many feel stress over how their bodies look. They may stay away from activities where the chest can be seen, such as swimming. They also might wear clothes that hide the dip in the chest.
Diagnosis
Diagnosis involves the steps that a healthcare professional takes to find out if you or your child has pectus excavatum. The healthcare professional starts by doing an exam of the chest. This may be enough to diagnose the condition. Other tests can check for health issues linked with pectus excavatum that affect the heart and lungs. These tests may include:
- Chest X-ray. This test can make images of the dip in the breastbone. It often shows the heart being pushed into the left side of the chest. X-rays take only a few minutes to do.
- CT scan or MRI. Each of these tests can help find out how serious the pectus excavatum is. They also can show whether the heart or lungs are being compressed. CT scans and MRI scans take many images from various angles to make detailed images of the organs and tissues in the body.
- Electrocardiogram. An electrocardiogram can show whether the heart's rhythm is regular or not. It also can show whether the electrical signals that control the heartbeat are timed properly. To do the test, a healthcare professional places sticky patches called electrodes on the chest. Wires connect the patches to a computer that prints or shows results.
- Echocardiogram. An echocardiogram can show real-time images of how well the heart and heart valves are working. To do the test, a healthcare professional presses a wand against the chest. The wand gives off sound waves that make pictures of the heart. An echocardiogram also shows whether the chest wall may be affecting heart function and the flow of blood through the heart.
- Lung function tests. These types of tests measure the amount of air that the lungs can hold. They also measure how quickly the lungs can push out air.
- Exercise function test. This test tracks how well the heart and lungs work during exercise, usually on a bike or treadmill.
Treatment
Pectus excavatum treatments include physical therapy, medical devices and surgery. Surgery is mainly for people who have moderate to severe symptoms. People who have mild symptoms may get better with other treatments.
Some treatments aim only to improve how the chest looks. For example, dermal fillers or silicone implants can help fill in the sunken part of the chest.
Therapies
Treatments that don't involve surgery may help some people with mild pectus excavatum. They include the following:
- Physical therapy. Some physical therapy exercises may improve posture and increase the degree to which the chest can expand.
- Sternal suction. This treatment for children and younger teens involves placing a cup- or bell-shaped device on the breastbone. The device uses suction to gently pull the breastbone forward. The device needs to be used for one or more hours a day for about 12 to 15 months.
Surgery or other procedures
Surgery to repair pectus excavatum can ease symptoms and improve how the chest looks. Surgery tends to be a treatment choice for teens and young adults. Surgery may be right for some older people too.
Two types of surgeries can repair pectus excavatum:
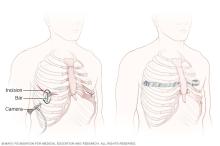
- Nuss procedure. This is the more common type of surgery. It's minimally invasive, meaning it's done through small cuts. In general, the surgeon makes small cuts on each side of the chest. The surgeon places long-handled tools and a tiny camera through the cuts. Then the surgeon threads a curved metal bar under the sunken breastbone. The bar is rotated to raise the breastbone into a more typical position. Often, more than one bar is used. The bars are removed after about two or three years.
- Ravitch technique. This older surgery is done much less often than the Nuss procedure. With the Ravitch technique, the surgeon makes a much larger cut down the center of the chest. The surgeon removes the deformed cartilage that attaches the ribs to the lower breastbone. Then the surgeon fixes the breastbone into a more regular position with surgical hardware. The hardware might include a metal strut or mesh supports. These supports are removed after a year or more.
Most people who have surgery to correct pectus excavatum are happy with the change in how their chests look. Studies found that to be true no matter which of the two surgeries people had.
Surgeons have many ways to help control pain from surgery. During surgery, they can freeze nerves to block pain after surgery. This is called cryoablation, and it can help with recovery. The pain-relieving effects may last for weeks.
Other treatments aim to improve only the appearance of the chest. These are called cosmetic treatments. They're mainly for people who have mild pectus excavatum without meaningful symptoms. A healthcare professional can place a silicon implant in the chest to fill in the sunken area. Or shots of certain dermal fillers may help fill in the area.
Coping and support
Most children and teens just want to fit in and look like their peers. This can be very hard for young people who have pectus excavatum. Counseling may help some kids and teens feel better about themselves. Online support groups and forums also are available. These can help connect kids and teens with other young people who have pectus excavatum.
Preparing for an appointment
If you or your child has pectus excavatum, you might first talk about the condition with your family healthcare professional. Then you might be referred to a doctor who does pediatric or chest surgery.
What you can do
You may want to write a list that includes:
- Detailed descriptions of your symptoms or your child's symptoms.
- Information about past health problems.
- Information about common health conditions in your family.
- All the medicines and supplements you or your child takes.
- Questions you want to ask the healthcare team, including what treatments are available.
What to expect from your doctor
Your healthcare professional may ask some of the following questions:
- When did these symptoms start?
- Have they become worse recently?
- Has anyone else in your family had pectus excavatum?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use