
Polycystic ovary syndrome (PCOS)
Conditions
Overview
Polycystic ovary syndrome (PCOS) is a hormone health issue that starts to show signs in people of childbearing age. If you have PCOS, you may not have periods very often. Or you may have periods that last many days. You also may have male-pattern hair growth, called hirsutism, which is too much of a group of hormones called androgens in your body.
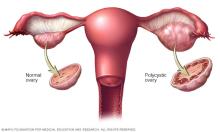
With PCOS, many small sacs of fluid may grow along the outer edge of the ovary. These are called cysts. Inside the small, fluid-filled cysts of PCOS are immature eggs. These are called follicles. These follicles are unable to regularly release eggs.
Although PCOS is named for these small cysts on the ovaries, the condition is driven by the effects of androgen and changes in how your body uses a hormone called insulin, which controls blood sugar.
The exact cause of PCOS is not known, but genetic and lifestyle factors may play a part. Early diagnosis and treatment along with weight management may lower the risk of long-term health issues, such as type 2 diabetes and heart disease.
Symptoms
Symptoms of polycystic ovary syndrome (PCOS), often start around the time of the first menstrual period. Sometimes symptoms develop later after you have had periods for a while.
The symptoms of PCOS vary and can change over time. Some people with PCOS may have very severe symptoms, while others have mild symptoms or no symptoms at all. A diagnosis of PCOS is made when you have at least two of these symptoms:
- Irregular periods. PCOS can cause your periods to be less predictable. You may skip periods or have periods that are very far apart. For example, you might have fewer than eight periods a year. And they may be more than 35 days apart. On the other hand, you may have periods that are heavy, last for many days or come more often than usual. You also may stop having periods or have trouble getting pregnant.
- Too much androgen effect. High levels or high activity of the hormones called androgens can cause extra hair on the face and body hair, often in places men typically grow hair. This is called hirsutism. It often shows up on the chin, sideburn area, chest, upper thighs or back. Sometimes, male-pattern hair loss on the head or severe acne can happen, too.
- Polycystic ovaries. Your ovaries might be slightly bigger than usual. You also might have many small, fluid-filled sacs around the edge of your ovaries. These sacs are called follicles and they hold immature eggs. But because the ovaries don't work the way they should, the eggs often don't get released. Large ovarian cysts are not a sign of PCOS.
PCOS symptoms are usually more serious in people with obesity.
When to see a doctor
See your healthcare professional if you're worried about your periods, if you're having trouble getting pregnant or if you have symptoms of too much androgen. These might include new hair growth on your face and body, acne, and male-pattern hair loss.
Causes
The exact cause of polycystic ovary syndrome (PCOS) isn't known. Most experts think there are many things that might play a role, including:
-
Insulin resistance. In PCOS, your body may not respond well to insulin. Insulin is a hormone made in the pancreas. It allows cells to use sugar, your body's main source of energy. If cells don't respond to insulin the way they typically would, blood sugar levels go up. Your body then makes more insulin to try to bring blood sugar levels down.
One symptom of insulin resistance is dark, velvety patches of skin on the lower part of the neck, armpits, groin or under the breasts. Feeling hungrier than usual and weight gain may be other symptoms.
- Genes. Some research shows that certain genes might be linked to PCOS. Having a family history of PCOS may mean you're more likely to have it.
- Too much androgen activity. With PCOS, your body may make too much of the androgen hormones, which are at higher levels in males. You also may have normal androgen hormone levels but the hormones are more active. This can cause male-pattern hair growth (hirsutism) and some kinds of acne. As a result, ovulation may not always happen. This means that eggs don't develop regularly and aren't released from the follicles where they develop.
Risk factors
Certain factors may increase the risk of PCOS, such as having family members who have PCOS. Being overweight or having obesity may put you at risk of PCOS. Insulin resistance and too much androgen activity also may contribute to the risk of PCOS.
Complications
Complications of polycystic ovary syndrome (PCOS) can include:
- Infertility. PCOS can make it harder to get pregnant. However, pregnancy is still possible and does happen for many people with the PCOS. If you don't wish to become pregnant, use pregnancy prevention methods such as birth control.
- Pregnancy complications. You might have a higher chance of getting diabetes during pregnancy, which is called gestational diabetes. You also may be more likely to have high blood pressure during pregnancy, miscarriage or early birth.
- Metabolic dysfunction-associated steatotic liver disease (previously called nonalcoholic fatty liver disease). This happens when fat builds up in your liver, which is a risk factor for cardiovascular disease.
- Metabolic syndrome. Metabolic syndrome is a group of health issues that often happen together. Metabolic syndrome can include high blood pressure, high fasting blood sugar, and unhealthy cholesterol or fats in your blood. These fats are called triglycerides. Having these can significantly increase your risk of heart disease and blood vessel issues.
- Type 2 diabetes or prediabetes. PCOS may cause you to have a greater chance of high blood sugar.
- Sleep apnea. This happens when you stop breathing for short periods of time while sleeping.
- Mental health issues. Depression, anxiety and eating disorders can happen with PCOS.
- Uterine and ovarian cancer. Some people with PCOS develop a condition that causes the uterus lining to become too thick. This increases the risk of cancer in the lining of the uterus, called endometrial cancer. Endometrial cancer is a type of uterine cancer. The risk of ovarian cancer also is higher in people with PCOS.
Obesity is common in people with PCOS and can make complications worse.
Diagnosis
There's no single test to diagnose polycystic ovary syndrome (PCOS). Your healthcare professional is likely to start by talking about your symptoms, medicines and other health issues. Your healthcare professional also may ask about your menstrual periods and any weight changes. A physical exam may be done. This includes checking for signs of male-pattern hair growth, insulin resistance and acne.
Your healthcare professional might then recommend:
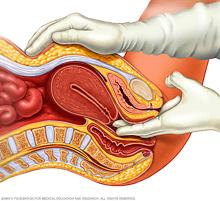
- Pelvic exam. During a pelvic exam, your healthcare professional can check your reproductive organs for masses, growths or other changes.
- Blood tests. Blood tests can measure hormone levels. These tests can help rule out other causes of health issues that may be mistaken for PCOS. You might have other blood tests, such as fasting cholesterol and triglyceride levels. A glucose test can measure how your body responds to sugar.
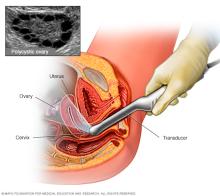
- Ultrasound. An ultrasound can look at your ovaries and the thickness of the lining of your uterus. A wandlike device is placed in your vagina. The device uses sound waves to create images on a computer screen.
If you are diagnosed with PCOS, your healthcare professional might recommend more tests for complications. These tests can include:
- Regular checks of blood pressure, glucose tolerance, and cholesterol and triglyceride levels.
- Screening for depression and anxiety.
- Screening for obstructive sleep apnea.
Treatment
There is no cure for polycystic ovary syndrome (PCOS). PCOS treatment focuses on managing symptoms and reducing the risk of long-term health issues, such as heart disease and diabetes. Your treatment plan will depend on your symptoms, current health issues and pregnancy goals. Usually, a combination of treatments such as lifestyle changes and medicine is recommended.
Lifestyle changes
To help manage polycystic ovary syndrome (PCOS), try to:
-
Stay at a healthy weight. Weight loss is recommended for people with PCOS and overweight or obesity. Your healthcare professional may suggest a low-calorie diet and regular exercise. Even losing a small amount of weight — for example, losing 5% of your body weight — can improve PCOS symptoms and reduce the risk of other health issues. For example, exercise can lower blood sugar levels by improving how insulin works in the body. It also can lower androgen levels and help you ovulate so that your periods are more regular.
Losing weight may help your medicines work better, and it can help with infertility. Ask your healthcare professional about a weight-control program, if your doctor thinks you need one. Meet with a registered dietitian for help reaching your weight-loss goals.
- Limit calories. When it comes to losing weight for people with PCOS and overweight or obesity, eating fewer calories is the most important thing — no matter what kind of diet you follow. Research hasn't shown that one diet works better than another for weight loss in PCOS, as long as you're eating fewer calories overall.
- Be active. Aerobic exercise and strength training helps lower blood sugar levels. If you have PCOS, getting more daily activity and regular exercise may treat or even prevent insulin resistance. Being active also may help you manage your weight and avoid diabetes.
Medicines to regulate periods
To make your periods more regular, your healthcare professional might recommend:
- Combination birth control pills. Pills that have both estrogen and progestin can help reduce androgen and make your menstrual cycle more regular. These medicines also can help lower your risk of endometrial cancer and improve irregular bleeding, unwanted hair growth and acne.
- Progestin therapy. Taking a progestin for 10 to 14 days every 1 to 2 months can regulate your periods and protect against endometrial cancer. Progestin therapies don't improve androgen levels and won't prevent pregnancy. The progestin-only mini pills or progestin-containing intrauterine device are better choices if you also wish to avoid pregnancy.
Medicines to treat infertility
Not everyone with PCOS has difficulty getting pregnant. If you're trying to get pregnant and have irregular periods or have not become pregnant within 6 to 12 months, your healthcare professional may suggest medicines to help you ovulate, such as:
- Metformin (Glumetza, Fortamet). This medicine for type 2 diabetes improves insulin's ability to lower blood sugar. If you have prediabetes, metformin may delay or prevent type 2 diabetes and help with weight loss.
- GLP-1 medicines, such as Ozempic or Zepbound. For some people with PCOS, GLP-1 medicines may be used to help lower blood sugar and promote weight loss. GLP-1 medicines are usually given as a shot. They are stopped before pregnancy.
- Letrozole (Femara). This treatment helps the body make more of a hormone needed to trigger ovulation.
- Clomiphene. This medicine is a pill that's taken at the beginning of your menstrual cycle. If you don't become pregnant using clomiphene, your healthcare professional might recommend adding metformin to help you ovulate.
- Gonadotropins. These hormone medicines are given as shots.
If needed, talk with your healthcare professional about procedures that may help you become pregnant. For example, in vitro fertilization may be an option.
Medicines to treat male-pattern hair growth or acne
To reduce male-pattern hair growth or improve acne, your healthcare professional might recommend:
- Birth control pills. These pills lower the amount of androgens made or reduce the activity of those hormones, which can help clear acne and reduce male-pattern hair growth.
- Spironolactone (Aldactone). This medicine blocks the effects of androgens on the skin, which can help reduce male-pattern hair growth and acne. Spironolactone can cause birth defects, so effective birth control is needed while taking this medicine. This medicine isn't recommended if you're pregnant or planning to become pregnant.
- Eflornithine (Vaniqa). This cream can slow facial hair growth.
- Hair removal. Electrolysis and laser hair removal are two hair removal options. Electrolysis places a tiny needle in each hair follicle. The needle sends out a pulse of electricity. The electricity destroys the follicle. Laser hair removal uses light energy to remove unwanted hair. You might need many treatments of electrolysis or laser hair removal. Shaving, plucking or using creams that dissolve unwanted hair also may help, but the results are temporary. Often hair removal and medicines are used together.
- Acne treatments. Medicines, including pills and creams or gels, may help improve acne. Talk to your healthcare professional about options.
Coping and support
Although there is no cure for polycystic ovary syndrome (PCOS), lifestyle changes and treatments can improve symptoms and reduce long-term health effects. To cope, try these strategies:
- Connect with others. Finding support from other people with PCOS can be helpful. Whether it's an online community, PCOS support group, or trusted friend or family member, sharing experiences can make you feel understood and less alone.
- Learn as much as you can. Learning about PCOS and how it affects your body can help you feel more empowered. Turn to reliable sources such as your healthcare team to better understand your diagnosis, symptoms and treatment.
- Prioritize your mental health. Living with a chronic condition like PCOS can be stressful. Sometimes, this can lead to feelings such as anxiety or depression. Talk openly with your care team about how you're feeling and don't be afraid to ask for help.
Living with PCOS is challenging and different for everyone. Not all people with PCOS will have the same symptoms or face the same health issues. Although PCOS does increase your risk of complications such as infertility or diabetes, it doesn't always mean these will happen.
Preparing for an appointment
For polycystic ovary syndrome (PCOS), you may see a specialist in female reproductive medicine, called a gynecologist. You also may see a specialist in hormone disorders, called an endocrinologist, or an infertility specialist, called a reproductive endocrinologist.
Here's some information to help you get ready for your appointment.
What you can do
Before your appointment, make a list of:
- Symptoms you've been having, and for how long.
- Information about your periods, including how often they happen, how long they last and how heavy they are.
- All medicines, vitamins, herbs and other supplements you take, including the amount and how often.
- Key personal and health information, including other health conditions, recent life changes and stressors.
- Questions to ask your healthcare professional.
Some basic questions to ask include:
- What tests do you recommend?
- How does PCOS affect my chance of getting pregnant?
- Are there any medicines that might help improve my symptoms or make it easier to get pregnant?
- Are there things I can do to improve my PCOS symptoms?
- How will PCOS affect my health later in life?
- I have other health issues. How can I manage them alongside PCOS?
Be sure to ask any other questions that you may have.
What to expect from your doctor
Your healthcare professional is likely to ask you a number of questions, including:
- What are your symptoms? How often do they happen?
- How bad are your symptoms?
- When did each symptom start?
- When was your last period?
- Have you gained weight since you first started having periods? How much weight did you gain, and when did you gain it?
- Does anything seem to improve your symptoms? Make them worse?
- Are you trying to get pregnant, or do you wish to become pregnant?
- Has any close blood relative, such as your mother or a sister, ever been diagnosed with PCOS?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use