
Ulcerative colitis
Conditions
Overview
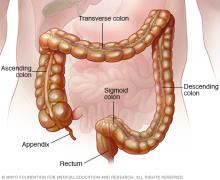
Ulcerative colitis is a type of inflammatory bowel disease (IBD) that causes inflammation and sores, called ulcers, in the colon. Ulcerative colitis (UL-sur-uh-tiv koe-LIE-tis) affects the innermost lining of the colon and rectum. The condition typically begins in the rectum and then may extend upward through part or all of the colon. The colon also is called the large intestine.
Ulcerative colitis symptoms usually develop over time, rather than starting suddenly. It is a chronic condition that sometimes can lead to life-threatening complications if not properly treated.
While there is no current cure with medicine, treatment can greatly reduce symptoms and heal the lining of the colon, which can lead to long-term remission.
Types
Healthcare professionals often classify ulcerative colitis according to its location. Types of ulcerative colitis include:
- Ulcerative proctitis. Inflammation is limited to the rectum. This is the area closest to the anus. Rectal bleeding or urgency may be the only sign of the disease. But constipation also can be a symptom.
- Left-sided colitis. In left-sided colitis, inflammation extends from the rectum up through the sigmoid colon and descending colon. Proctosigmoiditis is a type of left-sided colitis. Inflammation involves the rectum and sigmoid colon, which is the lower end of the colon. Symptoms of left-sided colitis include bloody diarrhea, belly cramps and pain, and not being able to pass stool despite the urge to do so, called tenesmus.
- Widespread colitis. This sometimes is called pancolitis. This type often affects the entire colon and causes bouts of bloody diarrhea that may be severe, belly cramps, and pain, fatigue and weight loss.
Crohn's disease and microscopic colitis are other conditions that cause inflammation in the digestive tract. Crohn's disease can affect any part of the gastrointestinal system, often including the small intestine, and it may involve deeper layers of the bowel wall. This differs from ulcerative colitis, which is limited to the colon and rectum.
Microscopic colitis, which includes lymphocytic and collagenous colitis, also can cause ongoing watery diarrhea, but it is different from ulcerative colitis. In microscopic colitis, the colon shows no signs of disease during colonoscopy, and inflammation is visible only under a microscope.
Symptoms
Ulcerative colitis symptoms can vary depending on how serious the inflammation is and where it is located. Symptoms may include:
- Diarrhea, often with blood, mucus or pus.
- Blood in the stool.
- Belly pain and cramping.
- Rectal pain.
- Urgency to pass stool.
- Not being able to pass stool despite urgency.
- Weight loss.
- Fatigue.
- Fever.
- In children, failure to grow.
About half the people with ulcerative colitis have mild to moderate symptoms. How ulcerative colitis affects people over time may vary. Some people have long periods without symptoms, called remission.
When to see a doctor
See a healthcare professional if you notice a change in your bowel habits that lasts a while or if you have symptoms such as:
- Belly pain.
- Blood in the stool.
- Ongoing diarrhea that doesn't get better with medicines you can get without a prescription.
- Diarrhea that awakens you from sleep.
- An unexplained fever that lasts more than a day or two.
Ulcerative colitis usually isn't fatal. But it's a serious disease that can cause life-threatening complications.
Causes
The cause of ulcerative colitis isn't known. In the past, diet and stress were thought to be causes. But today healthcare professionals understand that these factors may make symptoms worse rather than cause the disease. Stress, in particular, can affect the immune system and gut function. This may increase urgency to pass stool, diarrhea or belly pain during a flare.
Possible causes may include:
- Immune system issue. Something may go wrong with the immune system. When the immune system tries to fight off an invading virus or bacterium, an irregular immune response causes the immune system to attack the cells in the digestive tract too.
- Genetic traits. Several genetic markers have been associated with ulcerative colitis. Heredity also seems to play a role. The condition is more common in people who have family members with the disease. However, genetic testing is not helpful to diagnose or screen for the condition.
- Gut bacteria. The natural bacteria in the gut make up the gut microbiome. An imbalance in the gut microbiome may contribute to the immune response.
- Environmental factors. Where a person lives and other environmental influences such as diet and the use of antibiotics also may increase risk, though the exact role is still unclear.
Risk factors
Ulcerative colitis can happen to anyone. Risk factors may include:
- Age. Ulcerative colitis usually begins before the age of 30. But it can occur at any age, and some people may not develop the disease until after age 60.
- Race or ethnicity. Although white people have the highest risk of the disease, ulcerative colitis can happen in any race. The risk is even higher for those of Ashkenazi Jewish descent.
- Family history. You're at higher risk if you have a close relative, such as a parent, sibling or child, with the disease.
Complications
Possible complications of ulcerative colitis include:
- Severe bleeding.
- Severe dehydration.
- Loss of red blood cells, known as anemia.
- Bone loss, called osteoporosis.
- Inflammation of the skin, joints and eyes.
- An increased risk of colon cancer.
- A rapidly swelling colon, called toxic megacolon.
- Increased risk of blood clots in veins and arteries.
- Delayed growth and development in children.
Diagnosis
To diagnose ulcerative colitis, healthcare professionals do a colonoscopy and collect tissue samples, called biopsies, from the lining of the colon. Other types of tests such as stool tests, MRI and CT scans can help rule out complications or other forms of inflammatory bowel disease, such as Crohn's disease.
To help manage and decide on treatment for someone with ulcerative colitis, one or more of the following tests and procedures may be recommended.
Lab tests
- Blood tests. A healthcare professional may suggest blood tests to check for anemia or signs of infection. Anemia is a condition in which there aren't enough red blood cells to carry oxygen to the tissues. Sometimes, markers of inflammation also are checked.
- Stool studies. White blood cells or certain proteins in stool can suggest ulcerative colitis. A stool sample also can help rule out other conditions, such as infections caused by bacteria, viruses or parasites.
Endoscopic procedures
- Colonoscopy. This exam allows a healthcare professional to view the entire colon using a thin, flexible, lighted tube with a camera on the end. During the procedure, the healthcare professional takes samples of tissue for testing in a lab. This is called a biopsy. A tissue sample is necessary to make the diagnosis.
- Flexible sigmoidoscopy. Like colonoscopy, flexible sigmoidoscopy uses a thin, flexible, lighted tube with a camera on the end. But the tube is shorter. This test looks at the rectum and sigmoid colon — the lower end of the colon. If the colon is severely inflamed, this test may be done instead of a full colonoscopy.
Imaging procedures
- X-ray. If symptoms are severe, a standard X-ray of the abdominal area may be done to rule out dilation of the colon. Dilation of the colon can lead to serious complications, such as toxic megacolon and perforation.
- CT scan. A CT scan of the abdomen or pelvis may be done to help check for inflammation. It also may be done to rule out an abscess or other sources of pain.
- CT enterography and magnetic resonance (MR) enterography. A healthcare professional may recommend one of these noninvasive tests to exclude any inflammation in the small intestine. These tests are more sensitive for finding inflammation than are conventional imaging tests. MR enterography is a radiation-free alternative.
Treatment
Ulcerative colitis treatment involves medicines or surgery when medicines fail to control inflammation.
Several categories of medicines may be effective in treating ulcerative colitis. Medicines that work well for some people may not work for others, so it may take time to find a medicine that helps you. In addition, because some medicines have serious side effects, you need to weigh the benefits and risks of any treatment.
Treatment choices depend on how severe the disease is and where it occurs in the colon. In general, mild disease is often treated with aminosalicylates. Moderate disease may require corticosteroids, immunomodulators, biologic agents or small molecule medicines.
People with severe disease may need hospitalization for intravenous medicines, and they may need surgery if medicines do not work. The location of inflammation also matters. For example, rectal disease often responds well to topical treatments, while extensive colitis usually needs oral or intravenous medicines.
Medicines cannot cure ulcerative colitis, but they can control symptoms, reduce inflammation and help people stay in remission for long periods. The only true cure is surgery to remove the colon and rectum.
Anti-inflammatory medicines
Anti-inflammatory medicines often are the first step in the treatment of ulcerative colitis. They are used to calm inflammation in the colon and control symptoms. They include:
- Oral 5-aminosalicylates. These medicines are taken by mouth. Examples include sulfasalazine (Azulfidine), mesalamine (Apriso, Lialda, others) and balsalazide (Colazal). They often are taken long term to prevent flare-ups. Which one is recommended depends on the area of the colon that's affected. Some medicines also are available as an enema or suppository.
- Corticosteroids. These medicines, which include prednisone and budesonide, are generally reserved for moderate to severe ulcerative colitis that doesn't respond to other treatments. Corticosteroids are used to quickly control severe flares, but they are not safe for long-term use.
Immunomodulators
These medicines reduce inflammation by suppressing the immune system response that starts the process of inflammation. For some people, a combination of these medicines works better than one medicine alone.
Immunomodulators include:
- Azathioprine (Azasan, Imuran) and mercaptopurine (Purinethol, Purixan). These are the most widely used immunomodulators for the treatment of inflammatory bowel disease. Taking them requires that you follow up closely with your healthcare team and have your blood checked regularly to look for side effects, including effects on the liver and pancreas.
Biologic medicines
Also called biologics, this class of therapies targets proteins made by the immune system. Types of biologics used to treat ulcerative colitis include:
- Infliximab (Remicade), adalimumab (Humira) and golimumab (Simponi). These medicines, called tumor necrosis factor (TNF) inhibitors, work by neutralizing a protein produced by the immune system. They are for people with severe ulcerative colitis who don't respond to or can't tolerate other treatments.
- Vedolizumab (Entyvio). This medicine is approved for treatment of ulcerative colitis for people who don't respond to or can't tolerate other treatments. It works by blocking inflammatory cells from getting to the site of inflammation.
- Ustekinumab (Stelara). This medicine is approved for treatment of ulcerative colitis for people who don't respond to or can't tolerate other treatments. It works by blocking a protein that causes inflammation.
- Mirikizumab (Omvoh). Mirikizumab is a biologic medicine recently approved to treat ulcerative colitis.
- Risankizumab (Skyrizi). Risankizumab is another biologic medicine recently approved to treat ulcerative colitis.
- Guselkumab (Tremfya). This is the latest approved therapy in the same class as risankizumab and mirikizumab.
Small molecules
More recently, orally delivered agents also known as small molecules have become available for ulcerative colitis treatment. Types of small molecule medicines include:
- Tofacitinib (Xeljanz) and upadacitinib (Rinvoq). These medicines are known as Janus kinase (JAK) inhibitors. JAK inhibitors are small molecule medicines that help reduce inflammation by targeting parts of the immune system that cause inflammation in the intestines.
- Ozanimod (Zeposia) and etrasimod (Velsipity). These are another type of small molecule medicine available for ulcerative colitis. These are known as sphingosine 1-phosphate (S1P) receptor modulators.
Other medicines
You may need additional medicines to manage specific symptoms of ulcerative colitis. Always talk with your healthcare team before using medicines that you get without a prescription. One or more of the following medicines may be recommended:
- Antidiarrheal medicines. For severe diarrhea, loperamide (Imodium A-D) may be effective. Use antidiarrheal medicines with great caution and after talking with your healthcare team, because they may increase the risk of an enlarged colon, called toxic megacolon.
- Pain relievers. For mild pain, your care team may recommend acetaminophen (Tylenol, others). But not ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve) and diclofenac sodium. They can worsen symptoms and increase the severity of disease.
- Antispasmodics. Sometimes care professionals prescribe antispasmodic therapies to help with cramps.
- Iron supplements. If you have ongoing intestinal bleeding, you may develop iron deficiency anemia and be given iron supplements.
Surgery
Surgery for ulcerative colitis usually is needed if medicines no longer control the disease or if they cause serious side effects. Surgery also may be recommended if ulcerative colitis leads to complications, such as bleeding, colon rupture or cancer. The operation is called a proctocolectomy. A proctocolectomy removes the entire colon and rectum. This surgery cures ulcerative colitis.
In most cases, proctocolectomy involves another procedure called ileoanal anastomosis (J-pouch) surgery. A J-pouch eliminates the need to wear a bag to collect stool. The surgeon constructs a pouch from the end of the small intestine. The pouch is then attached directly to the anus, allowing for a relatively typical way to expel waste.
In some cases, a pouch is not possible. Instead, surgeons create a permanent opening in the belly, called an ileal stoma, through which stool is passed for collection in an attached bag.
In another type of procedure known as a continent ileostomy, also called a Kock pouch, the surgeon creates an ileal stoma opening in the belly, then places a one-way valve in the opening. A continent ileostomy does not collect stool in a bag. Instead, a tube is placed into the valve when stool needs to be emptied. This allows for control over the timing of bowel elimination.
Cancer surveillance
You will likely need more-frequent screening for colon cancer because of your increased risk. The recommended schedule depends on the location of your disease and how long you have had it. People with proctitis are not at increased risk of colon cancer.
If your disease involves more than your rectum, you will require a colonoscopy every 1 to 2 years, beginning as soon as eight years after diagnosis. The frequency depends on how much inflammation there is and how much of the colon is involved.
Lifestyle and home remedies
Sometimes you may feel helpless when facing ulcerative colitis. But changes in diet and daily habits can help manage symptoms and reduce the number of flare-ups. While these steps don't cure the disease, they can make living with ulcerative colitis easier.
Diet and nutrition
No single diet can prevent ulcerative colitis. Some foods and drinks even can make symptoms worse, especially during a flare. Keeping a food diary may help you spot patterns. If you notice that certain foods trigger symptoms, try avoiding them.
General suggestions include:
- Limit dairy products. Many people with ulcerative colitis are sensitive to lactose, which can cause gas, cramps and diarrhea. Using lactose-free products or enzyme supplements may help.
- Increase protein. Focus on eating protein-containing foods throughout the day. Examples include chicken, tofu, fish, turkey, eggs, yogurt, beans, chia seeds and nut butters.
- Eat smaller meals. Five or six small meals each day may be easier on your digestive system than a few large ones.
- Choose easy-to-digest foods. Soft, bland foods may reduce discomfort when symptoms are active. Avoid greasy, spicy or high-fiber foods if they make symptoms worse.
- Stay hydrated. Drink plenty of water. Limit caffeine, alcohol and carbonated drinks, which can worsen diarrhea and gas.
- See a dietitian. If you're losing weight or have limited food choices, a registered dietitian can help you maintain balanced nutrition.
Managing flares
Flares are times when ulcerative colitis symptoms return or get worse after a period of remission. While you cannot always prevent them, you can take steps to reduce their impact and support recovery.
- Stay in touch with your healthcare team. Regular communication with your care team is important. Contact your team if symptoms change or worsen.
- Keep up with recommended tests. Following your care team's advice for colonoscopies, blood work and other tests related to inflammatory bowel disease helps monitor disease activity and treatment effects.
- Track your symptoms. Writing down bowel habits, pain levels and other changes can help you and your team adjust treatment if needed.
- Support your nutrition. Ask about taking a multivitamin or mineral supplement, since ulcerative colitis can make it harder to absorb nutrients.
Handling stress
Stress does not cause ulcerative colitis. But it can make symptoms worse and possibly trigger flares. To reduce stress:
- Exercise regularly. Gentle activity, such as walking, can improve mood, strengthen bones and support bowel function.
- Practice relaxation techniques. Deep breathing, meditation, yoga or similar methods can calm the body.
- Seek support. Talking with a counselor or joining a support group can ease the emotional load of living with ulcerative colitis.
Alternative medicine
Many people with digestive diseases have used some form of complementary and alternative medicine. However, there are few well-designed studies showing the safety and effectiveness of complementary and alternative medicine.
Preparing for an appointment
Symptoms of ulcerative colitis may first prompt you to visit your primary healthcare professional. Your healthcare professional may recommend that you see a specialist who treats digestive diseases, called a gastroenterologist.
Here's some information to help you get ready for your appointment.
What you can do
When you make the appointment, ask if there's anything you need to do in advance, such as fasting before having a specific test. Make a list of:
- Your symptoms, including any that may not seem to be related to the reason for which you scheduled the appointment.
- Key personal information, including any major stresses or recent life changes.
- All medicines, vitamins or supplements you take, including the doses. Be sure to let your healthcare professional know if you're taking any herbal preparations as well.
- Questions to ask your doctor.
Take a family member or friend along, if possible, to help you remember the information you're given.
For ulcerative colitis, some basic questions to ask your doctor include:
- What's the most likely cause of my symptoms?
- Are there other possible causes for my symptoms?
- What kinds of tests do I need? Do these tests require any special preparation?
- Is this condition temporary or long lasting?
- What treatments are available, and which do you recommend?
- What types of side effects can I expect from treatment?
- Are there any prescription or over-the-counter medicines I need to avoid?
- What sort of follow-up care do I need? How often do I need a colonoscopy?
Other questions include:
- Are there any alternatives to the primary approach that you're suggesting?
- I have other health conditions. How can I best manage them together?
- Are there certain foods I can't eat anymore?
- Will I be able to keep working?
- Can I have children?
- Is there a generic alternative to the medicine you're prescribing?
- Are there any brochures or other printed material that I can take with me? What websites do you recommend?
What to expect from your doctor
Your doctor is likely to ask you several questions, such as:
- When did your symptoms start?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- Do you have abdominal pain?
- Have you had diarrhea? How often?
- Have you recently lost any weight without trying?
- Does anything seem to make your symptoms better?
- What, if anything, seems to make your symptoms worse?
Other questions include:
- Have you ever had liver problems, hepatitis or jaundice?
- Have you had any problems with your joints or eyes, had skin rashes or sores, or had sores in your mouth?
- Do you awaken from sleep during the night because of diarrhea?
- Have you recently traveled? If so, where?
- Is anyone else in your home sick with diarrhea?
- Have you taken antibiotics recently?
- Do you regularly take nonsteroidal anti-inflammatory drugs, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve)?
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use