
Pancreas transplant
Procedures
Overview
A pancreas transplant is a surgery to place a healthy pancreas from a deceased donor into a person whose pancreas no longer works properly.
The pancreas is an organ located behind the lower part of the stomach. One of the main jobs of the pancreas is to make insulin. Insulin is a hormone that regulates how sugar is absorbed into your cells.
If the pancreas doesn't make enough insulin, blood sugar levels can rise too high. This results in type 1 diabetes.
Most pancreas transplants are done to treat type 1 diabetes. A pancreas transplant can potentially cure this condition. But it's usually only for those with serious diabetes complications. This is because pancreas transplants can have significant side effects.
In some cases, pancreas transplants also may treat type 2 diabetes. Rarely, pancreas transplants may be used to treat pancreatic cancer, bile duct cancer or other cancers.
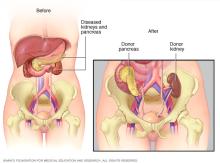
A pancreas transplant often is done with a kidney transplant in people whose kidneys have been damaged by diabetes.
Why it's done
A pancreas transplant can restore insulin production and improve blood sugar control in people with diabetes. But it is not a standard treatment option. The antirejection medicines needed after a pancreas transplant can have serious side effects.
Healthcare professionals may consider a pancreas transplant for people with any of the following:
- Type 1 diabetes that cannot be managed with standard treatment.
- Frequent insulin reactions.
- Ongoing concerns with blood sugar control.
- Severe kidney damage.
- Type 2 diabetes with both low insulin resistance and low insulin production.
A pancreas transplant is not commonly a treatment option for people with type 2 diabetes. That's because type 2 diabetes happens when the body becomes resistant to insulin or is not able to use it properly. Unlike type 1 diabetes, type 2 diabetes is not caused by a problem with the pancreas's insulin production.
However, for some people with type 2 diabetes who have both low insulin resistance and low insulin production, a pancreas transplant may be a treatment option. About 20% of all pancreas transplants in the U.S. are done in people with type 2 diabetes.
There are multiple types of pancreas transplants. These include:
- Pancreas transplant alone. People with diabetes who have early or no kidney disease may qualify for a pancreas transplant alone. A pancreas transplant surgery involves the placement of a healthy pancreas into a recipient whose pancreas is no longer working properly.
-
Combined kidney-pancreas transplant. Surgeons often do a pancreas transplant at the same time as a kidney transplant for people with diabetes who have or are at risk of kidney failure. This is called a combined or simultaneous kidney-pancreas transplant.
This approach aims to give you a healthy kidney and pancreas, reducing the risk of diabetes-related kidney damage in the future.
-
Pancreas-after-kidney transplant. For those facing a long wait for both a donor kidney and a donor pancreas, healthcare professionals may suggest a kidney transplant first if a donor kidney becomes available.
After you recover from kidney transplant surgery, you'll receive a pancreas transplant once a donor pancreas becomes available.
-
Pancreatic islet cell transplant. During pancreatic islet cell transplantation, insulin-producing islet cells are taken from a deceased donor's pancreas. The cells are injected into a vein that takes blood to your liver. You may need more than one injection of transplanted islet cells.
Pancreatic islet cell transplantation is approved by the Food and Drug Administration only for adults with type 1 diabetes who have frequent, severe low blood sugar issues despite treatment.
Risks
Complications of the procedure
Pancreas transplant surgery has a risk of serious complications. These include:
- Blood clots.
- Bleeding.
- Infection.
- High blood sugar or other metabolic health issues.
- Urinary complications, including leaking or urinary tract infections.
- Inflammation of the pancreas.
- Failure of the donated pancreas.
- Rejection of the donated pancreas.
Antirejection medicine side effects
After a pancreas transplant, you'll need to take medicines for the rest of your life to help prevent your body from rejecting the donor pancreas. These antirejection medicines can cause a variety of side effects, including:
- Bone thinning.
- High cholesterol.
- High blood pressure.
- Nausea, diarrhea or vomiting.
- Sensitivity to sunlight.
Other side effects may include:
- Puffiness.
- Weight gain.
- Swollen gums.
- Acne.
- Excessive hair growth or loss.
Antirejection medicines work by suppressing your immune system. These medicines also make it harder for your body to defend itself against infection and disease.
How you prepare
Choosing a transplant center
If your healthcare professional recommends a pancreas transplant, you'll be referred to a transplant center. You also can select a transplant center yourself or choose a center from your insurance company's list of preferred providers.
When you consider transplant centers, you may want to:
- Learn about the number and type of transplants the center performs each year.
- Ask about the transplant center's organ donor and recipient survival rates.
- Compare transplant center statistics through the database maintained by the Scientific Registry of Transplant Recipients.
- Consider other services provided by the transplant center, such as support groups, travel arrangements, local housing during recovery and referrals to other resources.
After you've chosen a transplant center, you'll need an evaluation to determine whether you meet the center's eligibility requirements.
When the transplant team looks at whether you qualify, they'll consider the following:
- Are you healthy enough to have surgery and to take post-transplant medicines for life?
- Do you have any medical conditions that would affect the success of the transplant?
- Are you willing and able to take medicines and follow the recommendations of the transplant team?
If you also need a kidney transplant, the transplant team will decide whether it's better for you to have the pancreas and kidney transplants at the same time, or to have the kidney transplant first, followed by the pancreas transplant later. The best option for you depends on the severity of your kidney damage, the availability of donors and your preference.
After you are accepted as a candidate for a pancreas transplant, your name will be added to a national list of people waiting for a transplant. The waiting time depends on your blood group and how long it takes to find a suitable donor whose blood and tissue types match yours.
About half of all adults waiting for a pancreas transplant wait a year or more. The average wait for a simultaneous kidney-pancreas transplant is about 1 to 3 years.
Staying healthy
Whether you're waiting for a donated pancreas to become available or your transplant surgery is already scheduled, it's important to stay as healthy as possible. This will increase your chances of a successful transplant.
- Take your medicines as prescribed.
- Follow any diet and exercise guidelines your care team gives you, and maintain a healthy weight.
- If you smoke, make a plan to quit. Talk to your healthcare team if you need help quitting.
- Keep all appointments with your healthcare team.
- Stay involved in healthy activities, including those that benefit your emotional health, such as relaxing and spending time with family and friends.
If you're waiting for a donor pancreas, make sure the transplant team knows how to reach you at all times.
The best outcomes occur when the pancreas is transplanted within 12 hours of organ recovery. Success is still possible beyond that, though waiting increases risks. Keep a packed hospital bag handy, and arrange for transportation to the transplant center in advance.
What you can expect
During the procedure
Surgeons perform pancreas transplants with general anesthesia. This means you are in a sleeplike state during the procedure. A member of the care team gives you the anesthesia medicine as a gas to breathe through a mask or as a liquid medicine injected into a vein.
After you're in a sleeplike state:
- A cut is made down the center of your abdomen.
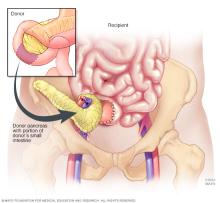
- The surgeon places the donor pancreas and a small portion of the donor's small intestine into your lower abdomen.
- The donor intestine is attached to either your small intestine or your bladder, and the donor pancreas is connected to blood vessels that also supply blood to your legs.
- Your own pancreas typically is left in place to aid digestion.
- If you also are receiving a kidney transplant, the blood vessels of the new kidney will be attached to blood vessels in the lower part of your abdomen.
- The new kidney's ureter, which is the tube that links the kidney to the bladder, will be connected to your bladder. Your own kidneys will stay in place unless they are causing high blood pressure, infection or other health concerns.
The surgical team monitors your heart rate, blood pressure and blood oxygen throughout the procedure.
Pancreas transplant surgery usually lasts about 4 to 6 hours. The total time depends on whether you are having a pancreas transplant alone or kidney and pancreas transplants at the same time.
After the procedure
After your pancreas transplant, you can expect to:
-
Stay in the intensive care unit for a couple of days. The healthcare team monitors your condition to watch for signs of complications. Your new pancreas should start working right away. If your old pancreas has been left in place, it continues to perform its other functions.
If you have a new kidney, it'll make urine just like your own kidneys did when they were healthy. Often this starts right away. But urine production may take up to a few weeks to return.
- Spend about a week in the hospital. Once you're stable, you're taken to a transplant recovery area. Expect soreness or pain around the incision site while you're healing.
- Have frequent checkups as you continue to recover. After you leave the hospital, close monitoring is necessary for 3 to 4 weeks. Your transplant team will develop a checkup schedule that's right for you. During this time, if you live in another town, you may need to stay close to the transplant center.
- Take medicines for the rest of your life. You'll take a number of medicines after your pancreas transplant. Medicines called immunosuppressants help keep your immune system from attacking your new pancreas. Additional medicines may help reduce the risk of other complications, such as infection and high blood pressure, after your transplant.
Results
After a successful pancreas transplant, your new pancreas will make the insulin your body needs. This means you'll no longer need insulin therapy to treat type 1 diabetes.
But even with the best possible match between you and the donor, your immune system will try to reject your new pancreas.
To avoid rejection, you'll need antirejection medicines to suppress your immune system. You'll likely take these medicines for the rest of your life. Since these medicines can make your body more prone to infection, your healthcare team also may prescribe antibacterial, antiviral and antifungal medicines.
Signs and symptoms that your body might be rejecting your new pancreas include:
- Belly pain.
- Fever.
- Excessive tenderness at the transplant site.
- Increased blood sugar levels.
- Vomiting.
- Decreased urination.
If you have any of these symptoms, notify your transplant team right away.
It's common for people who receive a pancreas transplant to have an acute rejection episode within the first few months after the procedure. An acute rejection episode happens when your body's immune system quickly and strongly tries to attack your new pancreas because it sees it as a foreign object. If this happens to you, you'll need to return to the hospital for treatment with strong antirejection medicine.
Pancreas transplant survival rates
Survival rates vary by procedure type and transplant center. The Scientific Registry of Transplant Recipients keeps current statistics for all U.S. transplant centers.
People who receive pancreas-only transplants have slightly higher rejection rates. It's unclear why results are better for those who receive a kidney and pancreas at the same time. Some research suggests that it may be because it's more difficult to monitor and detect rejection of a pancreas alone versus a pancreas and a kidney.
If your new pancreas fails, you can resume insulin treatments and consider a second transplant. This choice will depend on your current health, your ability to withstand surgery and your quality of life expectations.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use