
Hemochromatosis
Conditions
Overview
Hemochromatosis is a type of iron overload disease that's caused by a gene change passed down in families. Iron overload disease is any condition that causes the body to hold onto too much iron. Iron overload diseases include the following:
-
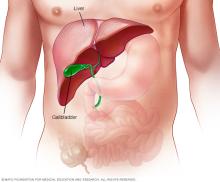
Hemochromatosis, also called primary or hereditary hemochromatosis, is the most common iron overload disease. It is a genetic condition that triggers the intestines to absorb too much iron from food. The excess iron is stored in the organs, especially the liver, heart and pancreas. Too much iron can damage the organs and lead to life-threatening conditions, such as liver disease, heart conditions and diabetes.
Families of Northern European descent have a higher genetic risk of hereditary hemochromatosis when both parents carry the gene change, also called a gene mutation. Only a few people who have the gene mutation ever develop serious complications.
- Secondary iron overload, sometimes called secondary hemochromatosis, is not passed on in families. It can be caused by another condition that causes the intestines to absorb too much iron, such as liver disease or too much alcohol. Or it can happen when you get too much iron, such as from too many blood transfusions. Over time, secondary iron overload can damage organs too.
Hemochromatosis is different from hemosiderosis. Hemosiderosis means iron has started to collect in body tissues but hasn't yet caused organ damage. These conditions also are different from simply having high iron. "High iron" is a term that usually refers to a blood test showing higher than typical iron levels. But that doesn't necessarily mean iron has built up in the organs.
Treatment for hemochromatosis usually includes removing blood from the body on a regular basis. This lowers iron levels because much of the body's iron is contained in red blood cells.
Symptoms
Some people with hemochromatosis never have symptoms. They may be diagnosed based on a routine blood test, sometimes done because of family history of the condition.
Early signs and symptoms
Early signs and symptoms of iron overload, including symptoms of hereditary hemochromatosis, often overlap with those of other common conditions. They may include:
- Weakness.
- Tiredness.
- Joint pain.
- Belly pain.
These symptoms can happen to anyone with hemochromatosis. But there are some differences in symptoms based on sex assigned at birth.
Symptoms of hemochromatosis in males:
- Loss of sex drive.
- Not being able to get and keep an erection firm enough for sexual activity, also called impotence.
Symptoms of hemochromatosis in females:
- Missing menstrual periods.
- Symptoms usually appear later in life. This may happen because iron is lost through menstruation and pregnancy. So less iron is stored in the body. After menopause or hysterectomy, this changes.
Other signs and symptoms
Symptoms of iron overload, including symptoms of hereditary hemochromatosis, also can include:
- Diabetes.
- Heart problems and conditions, such as heart rhythm changes and heart failure.
- Liver failure.
- Visible skin changes, including bronze or gray skin color. The term "bronze diabetes" is sometimes used when a person has both type 2 diabetes and a bronze skin color.
- Eye changes that affect vision.
When symptoms typically appear
The most common type of hemochromatosis is present at birth. But most people don't have symptoms until later in life. For men, symptoms usually start after age 40. Women are more likely to have symptoms after menopause or after age 60.
When to see a doctor
See a healthcare professional if you have any of the symptoms of hemochromatosis. If you have a parent, sibling or child who has hemochromatosis, ask your healthcare team about genetic testing. Genetic testing can check if you have the gene that increases your risk of hemochromatosis.
Causes
Hemochromatosis, also called hereditary hemochromatosis, is a type of genetic iron overload disease caused by a gene change, also called a gene mutation. The gene change is passed down in families. This is by far the most common type of iron overload disease.
Other types of iron overload are not genetic. They may be called secondary iron overload or acquired iron overload.
Genetic causes of hemochromatosis
Hereditary hemochromatosis can be caused by mutations to different genes that control the amount of iron the body absorbs from food.
- HFE gene. A gene called HFE is most often the cause of hereditary hemochromatosis. This is the type of hemochromatosis that mostly affects adults in midlife. The HFE gene has two common mutations, C282Y and H63D.
- HJV, HAMP or TFR2 genes. A mutation in any of these genes can cause a type of hemochromatosis called juvenile hemochromatosis. Juvenile hemochromatosis affects young people. It causes the same symptoms that hereditary hemochromatosis causes adults. But iron buildup begins earlier, so symptoms usually appear between the ages of 15 and 30.
If you inherit one gene mutation from each parent, you may develop hemochromatosis. You also can pass the altered gene on to your children. But not everyone who inherits two mutated genes develops symptoms linked to the iron overload of hemochromatosis.
If you inherit a gene mutation from one parent, you're not likely to develop hemochromatosis. But you are considered a carrier and can pass the altered gene on to your children. Your children won't develop the disease unless they also inherited another altered gene from the other parent.
Causes of secondary or acquired iron overload
Some iron overload is not caused by a gene change passed on in families. Examples include the following:
- Neonatal hemochromatosis is a serious disease where iron builds up quickly in the liver of a baby while in the womb. It is thought to be an autoimmune disease, in which the body attacks itself.
- Secondary iron overload can be caused by another condition that causes the intestines to absorb too much iron, such as liver disease, or by too much alcohol. Or it can be caused by too much iron in the body, such as from too many blood transfusions to treat anemia or other conditions. Less often, secondary iron overload can happen from taking too much of an iron supplement.
Diet alone usually does not cause iron overload. But, rarely, some people of African and African American descent may be at increased risk from a diet too high in iron. This is likely due to a gene change passed down in families.
How iron overload affects the organs
Iron plays an important role in several body functions, including helping to produce blood. But too much iron is toxic.
A hormone secreted by the liver, called hepcidin, controls how iron is used and absorbed in the body. It also controls how excess iron is stored in various organs. In hemochromatosis, the role of hepcidin is affected, causing the body to absorb more iron than it needs.
In other iron overload disease, the body does not absorb too much iron from food. Instead, it usually happens from too many blood transfusions.
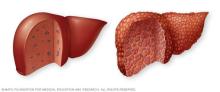
In hemochromatosis and other iron overload disease, excess iron is stored in major organs, especially the liver. Over a period of years, the stored iron can cause severe damage that may lead to organ failure. It also can lead to long-lasting diseases, such as cirrhosis, diabetes and heart failure. Many people have gene changes that cause hemochromatosis. However, not everyone develops iron overload to a degree that causes tissue and organ damage.
Risk factors
Factors that increase the risk of hemochromatosis include:
- Having two copies of an altered HFE gene. This is the greatest risk factor for hereditary hemochromatosis.
- Family history. Having a parent or sibling with hemochromatosis increases the likelihood of developing the disease.
- Ethnicity. People of Northern European descent are more prone to hereditary hemochromatosis than are people of other ethnic backgrounds.
- Sex assigned at birth. Males are more likely than females to have symptoms of hemochromatosis at an earlier age. Because females lose iron through menstruation and pregnancy, they tend to store less of the mineral. After menopause or a hysterectomy, the risk goes up for females.
Complications
Untreated, hemochromatosis and iron overload can lead to several complications. These complications especially affect the joints and organs where excess iron tends to be stored, such as the liver, pancreas and heart. Complications can include:
- Liver issues. Cirrhosis is permanent scarring of the liver. It is just one of the complications that may happen. Cirrhosis increases the risk of liver cancer and other life-threatening complications.
- Diabetes. Damage to the pancreas can lead to diabetes.
- Heart conditions. Excess iron in the heart affects the heart's ability to circulate enough blood for the body's needs. This is called congestive heart failure. Hemochromatosis also can cause irregular heart rhythms, called arrhythmias.
- Reproductive problems. Excess iron can lead to erectile dysfunction and loss of sex drive in males. It can cause an absence of the menstrual cycle in females.
- Skin color changes. Deposits of iron in skin cells can make the skin appear bronze or gray in color.
Diagnosis
Diagnosis and tests
Hemochromatosis and iron overload can be difficult to diagnose. Early symptoms such as stiff joints and fatigue are commonly caused by other conditions.
Many people with the disease don't have any symptoms other than high levels of iron in their blood. Hemochromatosis may be identified because of irregular blood test results after testing is done for other reasons.
Diagnosis criteria on what's considered iron overload can differ depending on where testing is done. But when blood test results are higher than expected, a genetic test may be done to check for the gene mutation that causes hereditary hemochromatosis. This test also may be done when screening family members of people diagnosed with the disease.
An MRI or liver biopsy may be done to check iron levels in the liver and check for organ damage, if suspected.
Blood tests
There's no single hemochromatosis blood test. But a number of blood tests, sometimes called labs, may be done to screen for iron overload. Two key tests to screen for iron overload are:
- Serum transferrin saturation. This test measures the amount of iron bound to the protein transferrin that carries iron in the blood. Different testing laboratories use different values of what's too high. But a transferrin saturation value of 45% or more often is considered too high. If high, a serum ferritin test may be done.
- Serum ferritin.This test measures the amount of iron stored in the liver. Different testing laboratories use different values of what's too high. But a value of more than 200 or 300 micrograms per liter often is considered high for people assigned male at birth. And more than 150 or 200 micrograms per liter often is considered high for people assigned female at birth.
These blood tests for iron may be done after fasting. Elevations in one or all of these tests can be found in other conditions. You may need to have the tests repeated for the most accurate results.
Additional testing
A healthcare professional may suggest other tests to confirm the diagnosis and to look for other problems:
- Liver function tests. These tests can help identify liver damage.
- MRI and ultrasound. An MRI is a fast and noninvasive way to measure the degree of iron overload in the liver. This test may be done to check iron levels in the liver and confirm organ damage, if suspected. Sometimes MRI is combined with ultrasound in a test called magnetic resonance elastography. Or ultrasound is done alone. These tests help measure how stiff liver tissue is from scarring.
- Genetic test. Testing DNA for changes in the HFE gene is recommended if there are high levels of iron in the blood. If you're considering genetic testing for hemochromatosis, discuss the reasons for and against testing with your healthcare professional or a genetic counselor.
- Removing a sample of liver tissue for testing. If liver damage is suspected, a liver biopsy may be done. During a liver biopsy, a sample of tissue is removed from the liver using a thin needle. The sample goes to a lab to be checked for the presence of iron. The lab also looks for evidence of liver damage, especially scarring or cirrhosis. Risks of biopsy include bruising, bleeding and infection.
Screening healthy people for hemochromatosis
Genetic testing is recommended for all parents, siblings and children of anyone diagnosed with hemochromatosis. If a gene change is found in only one parent, then children do not need to be tested.
Treatment
There is no cure for hemochromatosis. But hemochromatosis treatments, which are the same as other iron overload treatments, can help manage the condition and stop it from causing more harm. They include:
- Blood removal. This is also called therapeutic phlebotomy.
- Medicine to remove extra iron from the body, but only if phlebotomy is not an option for you. This treatment is called chelation.
- Dietary changes. To reduce the risk of complications from hemochromatosis, do not take iron supplements or vitamin C supplements. And do not eat raw seafood. If you have liver damage, cut out alcohol completely. Other foods with iron usually are OK.
Blood removal
Medical professionals can treat hemochromatosis safely and effectively by removing blood from the body on a regular basis. The process, called therapeutic phlebotomy, is similar to blood donation.
The goal is to lower iron levels. Phlebotomy lowers iron levels because much of the body's iron is contained in red blood cells. The amount of blood removed and how often it's removed depend on age, overall health and the severity of iron overload.
Side effects are usually mild. They mainly include symptoms that last a short time after phlebotomy. These may include feeling dizzy or like you might faint, nausea, vomiting, sweating, rapid breathing, or low blood pressure. You also may have bruising in the area where the needle is placed in your arm.
- Initial treatment schedule. In the beginning, around a pint (about 470 milliliters) of blood may be taken once or twice a week — usually in a hospital or medical professional's office. You lean back in a chair while a needle is placed into a vein in the arm. The blood flows from the needle into a tube that's attached to a blood bag.
- Maintenance treatment schedule. Once iron levels go down, blood can be removed less often, typically every 2 to 4 months. Some people may need to have blood removed more or less often. The schedule depends on how quickly iron builds up in the body. Some people may maintain typical iron levels without having any blood taken.
Donating blood is not a replacement for therapeutic phlebotomy. This is because your healthcare professional needs to test your iron levels and adjust phlebotomy treatments as needed.
Treating hemochromatosis can help relieve symptoms of tiredness, heart changes and skin darkening. It can help prevent serious complications such as liver disease, heart disease and diabetes. If you already have one of these conditions, phlebotomy may slow the progression of the disease.
Phlebotomy can't reverse joint pain, but it can slow the progression.
For someone with cirrhosis, a healthcare professional may recommend occasional screening for liver cancer. This usually involves an abdominal ultrasound and CT scan.
Chelation for those who can't undergo blood removal
Phlebotomy may not be an option for someone who has certain conditions, such as some anemias or heart complications. Instead, a healthcare professional may suggest a medicine, such as deferoxamine (Desferal) or deferasirox (Exjade, Jadenu), to remove excess iron. The medicine binds excess iron, allowing the body to get rid of iron through urine or stool in a process called chelation (kee-LAY-shun). Chelation medicines can be injected into the body or taken as a pill. Chelation is not commonly used in hemochromatosis.
Preparing for an appointment
Make an appointment with someone on your primary healthcare team if you have any symptoms that worry you. You may be referred to a specialist in digestive diseases, called a gastroenterologist, or to another specialist, depending on your symptoms. Here's some information to help you get ready for your appointment, and what to expect.
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your diet.
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Write down key personal information, including any major stresses or recent life changes. Learn if you have any liver disease in your family by asking your family members, if possible.
- Make a list of all medicines, vitamins or supplements that you're taking.
- Take a family member or friend along to help you remember what's been discussed.
- Write down questions to ask during your appointment.
Questions to ask your doctor
Some basic questions to ask include:
- What's the most likely cause of my symptoms?
- What kinds of tests do I need?
- Is my condition temporary, or will I always have it?
- What treatments are available? And what do you suggest for me?
- I have other health conditions. How can I best manage these conditions together?
- Are there any restrictions that I need to follow?
- Are there any brochures or other printed material that I can take with me? What websites do you recommend?
Don't hesitate to ask other questions during your appointment.
What to expect from your doctor
Be ready to answer questions your care team may ask:
- When did your symptoms start?
- Have your symptoms been continuous, or do they come and go?
- How severe are your symptoms?
- Does anything seem to improve your symptoms?
- What, if anything, appears to make your symptoms worse?
- Does anyone in your family have hemochromatosis?
- How many alcoholic beverages do you drink in a week?
- Are you taking iron supplements or vitamin C?
- Do you have a history of viral hepatitis, such as hepatitis C?
- Have you had blood transfusions before?
Stages
Hereditary hemochromatosis has three stages.
- Stage 1. In this earliest stage, you carry two copies of the inherited genes that can cause hemochromatosis. But lab tests show iron levels in the body are within a healthy range. Many people do not move beyond this stage.
- Stage 2. In this middle stage, your lab tests show signs of extra iron in the body. But there are no signs that the iron overload levels have caused tissue or organ damage.
- Stage 3. In this latest stage, you have signs of either tissue injury or organ damage related to iron overload.
Organ damage
Hemochromatosis is often diagnosed based on blood tests that show high ferritin levels or a gene mutation. Because of this, treatment begins early and can prevent organ damage.
When diagnosed later or without treatment, organ damage can happen. The liver is usually the first organ to be damaged. Too much iron can cause serious scarring of the liver, a condition called cirrhosis. A ferritin level higher than 1,000 micrograms per liter increases the risk of cirrhosis. Cirrhosis also increases the risk of liver cancer.
After liver damage happens, other organs can become damaged. Damage to the pancreas is what causes the changes in skin color, sometimes called bronze diabetes. Later, hemochromatosis may lead to heart damage. In juvenile hemochromatosis, however, heart damage may be one of the first signs.
Treatment is most successful when it begins before organ damage starts. If organ damage has happened, treatment can still help keep damage from getting worse. And sometimes it can help reverse some damage. For example, diabetes may improve or be reversed. And some liver scarring may improve. However, once cirrhosis is present, it often cannot be reversed.
Survival rates
If hemochromatosis is caught and treated early, before it causes serious damage, you often can live a full life. But if left untreated — especially if it leads to advanced stages of liver scarring, called cirrhosis, or heart conditions — life can be significantly shorter.
Many factors can affect how the condition progresses, also called the prognosis.
- Sex assigned at birth. Males tend to get symptoms earlier and have more severe complications.
- Age at time of diagnosis. Getting a diagnosis at the age of 56 or older is associated with a worse prognosis.
- How much iron has built up in the body. If your serum ferritin level is less than 2,000 micrograms per liter at the time you're diagnosed, your lifespan is likely to be similar to that of the general population.
- How early you're diagnosed. If phlebotomy treatment starts before cirrhosis or diabetes start, you often can live a full life.
- If you have cirrhosis. If you have cirrhosis, especially if it's at an advanced stage, it's associated with a worse prognosis and shorter lifespan.
- Inherited HFE gene mutation. The risk of death from a type of liver cancer called hepatocellular carcinoma is higher if you have hemochromatosis caused by the HFE gene. However, your risk of this type of cancer is highest if you already have cirrhosis.
- Alcohol use. When you have hemochromatosis, use of alcohol increases the risk of death. Alcohol may increase blood-iron level.
Phlebotomy treatment itself improves survival, even if you have organ damage. And with treatment, some organ damage is reversible once iron is removed from the body. Cirrhosis usually does not reverse, but liver scarring may improve. And treatment can slow or reverse other complications, such as diabetes and other liver disease.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use