
Inguinal hernia
Conditions
Overview
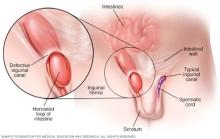
An inguinal hernia happens when tissue, such as part of the intestine, pokes through a weak spot in the abdominal muscles. The resulting bulge can be painful, especially when coughing, bending over or lifting a heavy object. However, many hernias do not cause pain.
An inguinal hernia isn't necessarily dangerous, but it doesn't get better on its own. It also can lead to life-threatening complications. A healthcare professional is likely to recommend surgery to fix an inguinal hernia that's painful or getting bigger. Inguinal hernia repair is a common surgical procedure.
Symptoms
Inguinal hernia symptoms include:
- A bulge in the area on either side of the pubic bone, which becomes more obvious when upright, especially when coughing or straining.
- A burning or aching sensation at the bulge.
- Pain, discomfort or pressure in the groin, especially when bending over, coughing or lifting.
- Occasionally, pain and swelling around the testicles when the protruding intestine descends into the scrotum.
Symptoms in children
Inguinal hernias in newborns and children result from a weakness in the abdominal wall that's present at birth. Sometimes the hernia will be seen only when a baby is crying, coughing or straining during a bowel movement. The baby might be irritable and have less appetite than usual.
In an older child, a hernia is likely to be more noticeable when the child coughs, strains during a bowel movement or stands for a long period.
Signs of trouble
If a hernia can't be pushed in, the contents of the hernia may be trapped in the abdominal wall. This is known as an incarcerated hernia. An incarcerated hernia can become strangulated, which cuts off the blood flow to the tissue that's trapped. A strangulated hernia can be life-threatening if it isn't treated.
Symptoms of a strangulated hernia include:
- Nausea, vomiting or both.
- Fever.
- Sudden pain that quickly gets worse.
- A hernia bulge that turns red, purple or dark.
- Not being able to move the bowels or pass gas.
When to see a doctor
Seek care right away if a hernia bulge turns red, purple, or dark or if you notice any other symptoms of a strangulated hernia.
See a healthcare professional if you have a painful or noticeable bulge in your groin on either side of your pubic bone. The bulge is likely to be more noticeable when you're standing, and you usually can feel it if you put your hand directly over the affected area.
Causes
Some inguinal hernias have no apparent cause. Others might happen because of:
- Increased pressure within the abdomen.
- A preexisting weak spot in the abdominal wall.
- Straining during bowel movements or urination.
- Strenuous activity, such as heavy lifting and standing or walking for many hours each day.
- Pregnancy.
- Coughing or sneezing often.
In many people, the abdominal wall weakness that leads to an inguinal hernia happens before birth when a weakness in the abdominal wall muscle doesn't close properly. Other inguinal hernias form later in life when muscles weaken or break down due to aging, strenuous physical activity or coughing that accompanies smoking.
Weaknesses also can happen in the abdominal wall later in life, especially after an injury or abdominal surgery.
In men, the weak spot usually occurs in the inguinal canal, where the spermatic cord enters the scrotum. In women, the inguinal canal carries a ligament that helps hold the uterus in place, and hernias sometimes happen where connective tissue from the uterus attaches to tissue surrounding the pubic bone.
Risk factors
Factors that contribute to forming an inguinal hernia include:
- Being male. Men are 8 to 10 times more likely to have an inguinal hernia than are women.
- Being older. Muscles weaken as you age.
- European ancestry. Studies show that people of European ancestry, often referred to as white, may be more likely to get inguinal hernias than people of other racial or ethnic backgrounds.
- Family history. You have a close relative, such as a parent or sibling, who has the condition.
- Long-lasting cough, such as from smoking.
- Long-lasting constipation. Constipation causes straining during bowel movements.
- Pregnancy. Being pregnant can weaken the abdominal muscles and cause increased pressure inside the abdomen.
- Premature birth and low birth weight. Inguinal hernias are more common in babies who are born prematurely or with a low birth weight.
- Having a connective tissue condition, such as Ehlers-Danlos syndrome or Marfan syndrome.
- Having a prostatectomy, which is the surgical removal of the prostate gland.
- Previous inguinal hernia or hernia repair. Having a previous hernia in childhood increases the risk of forming another inguinal hernia later in life.
Complications
Complications of an inguinal hernia include:
- Pressure on surrounding tissues. Most inguinal hernias enlarge over time if not repaired surgically. In men, large hernias can extend into the scrotum, causing pain and swelling.
- Incarcerated hernia. If the contents of the hernia become trapped in the weak point in the abdominal wall, the contents can block the bowel, leading to:
- Severe pain.
- Nausea or vomiting.
- Not being able to have a bowel movement or pass gas.
- Strangulation. An incarcerated hernia can cut off blood flow to part of the intestine. Strangulation can lead to the death of the affected bowel tissue. A strangulated hernia is life-threatening and requires immediate surgery.
Prevention
You can't prevent the congenital defect that increases your risk of an inguinal hernia. You can, however, reduce strain on your abdominal muscles and tissues. For example:
- Maintain a healthy weight. Talk to a healthcare professional about the best exercise and diet plan for you.
- Emphasize high-fiber foods. Fruits, vegetables and whole grains contain fiber that can help prevent constipation and straining.
- Lift heavy objects carefully or avoid heavy lifting. If you must lift something heavy, always bend from your knees — not your waist.
- Stop smoking. Besides its role in many serious diseases, smoking often causes a long-lasting cough that can lead to an inguinal hernia or make an existing one worse.
Diagnosis
A physical exam is usually all that's needed to diagnose an inguinal hernia. A healthcare professional will check for a bulge in the groin area. Because standing and coughing can make a hernia more prominent, you'll likely be asked to stand and cough or strain.
If the inguinal hernia isn't readily seen, a care professional might order an imaging test, such as an abdominal ultrasound, CT scan or MRI.
Treatment
If the hernia is small and isn't causing problems, a healthcare professional might recommend watchful waiting. Sometimes, wearing a supportive truss may help relieve symptoms. A health professional can help make sure the truss fits properly and is being used appropriately. In children, a care professional might try applying manual pressure to reduce the bulge before considering surgery.
Hernias that are painful or getting bigger usually need surgery to relieve discomfort and prevent serious complications.
There are two general types of hernia operations — open hernia repair and minimally invasive hernia repair.
Open hernia repair
In this procedure, the surgeon makes a cut in the groin and pushes the protruding tissue back into the abdomen. The surgeon then sews the weakened area, often reinforcing it with a synthetic mesh. This is called a hernioplasty. The opening is then closed with stitches, staples or surgical glue. Open hernia repair might be done with local anesthesia and sedation or general anesthesia.
After the surgery, you'll be encouraged to move about as soon as possible, but it might be several weeks before you're able to resume regular activities.
Minimally invasive hernia repair
In this procedure requiring general anesthesia, the surgeon operates through several small cuts in the belly. The surgeon may use laparoscopic or robotic instruments to repair the hernia. Gas is used to inflate the belly to make the internal organs easier to see.
A small tube with a tiny camera, called a laparoscope, is placed into one cut. Guided by the camera, the surgeon places tiny instruments through other small cuts and repairs the hernia using synthetic mesh.
People who have a minimally invasive repair might have less discomfort and scarring after surgery and a quicker return to regular activities. Long-term results of laparoscopic and open hernia surgeries are about the same.
Minimally invasive hernia surgery allows the surgeon to avoid scar tissue from an earlier hernia repair, so it might be a good choice for people whose hernias come back after open hernia surgery. It also might be a good choice for people with hernias on both sides of the body, called bilateral hernias.
As with open surgery, it may be a few weeks before you can get back to your usual activity level.
Preparing for your appointment
You'll likely start by seeing someone on your primary healthcare team. Here's some information to help you get ready for your appointment.
What you can do
Make a list of:
- Your symptoms, including when they started and how they may have changed or worsened over time.
- Key personal information, including recent life changes and family medical history.
- All medicines, vitamins or supplements you take, including doses.
- Questions to ask during your appointment.
Take a family member or friend along, if possible, to help you remember the information discussed during the appointment.
For an inguinal hernia, some basic questions to ask include:
- What's the most likely cause of my symptoms?
- What tests do I need?
- What treatments are available, and which one do you recommend for me?
- If I need surgery, what will my recovery be like?
- I have other health conditions. How can I best manage these conditions together?
- What can I do to prevent another hernia?
Don't hesitate to ask other questions you may have.
What to expect from your doctor
You'll likely be asked a few questions, such as:
- When did your symptoms begin?
- Have your symptoms stayed the same or gotten worse?
- Do you have pain in your abdomen or groin? Does anything make the pain feel worse or better?
- What physical activity do you perform on your job? What other physical activities do you regularly engage in?
- Do you have a history of constipation?
- Have you had a previous inguinal hernia?
- Do you or did you smoke? If so, how much?
What you can do in the meantime
Get emergency medical care if you have nausea, vomiting or fever or if your hernia bulge turns red, purple or dark.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use