
Intussusception
Conditions
Overview
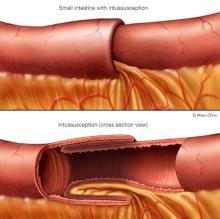
Intussusception (in-tuh-suh-SEP-shun) is a serious condition in which part of the intestine slides into another part, much like a telescope. This telescoping action often blocks food or fluid from passing through. Intussusception also cuts off the blood supply to the part of the intestine that's affected. This can lead to infection, death of bowel tissue or a tear in the bowel, called perforation.
Intussusception is the most common cause of intestinal blockage in children younger than 3 years old. The cause of most cases of intussusception in children is unknown. Though intussusception is rare in adults, most cases of adult intussusception are the result of an underlying medical condition, such as a tumor.
In children, the intestines can usually be pushed back into position with a minor procedure. In adults, surgery is often needed to correct the problem.
Symptoms
Children
The first sign of intussusception in an otherwise healthy baby may be sudden, loud crying caused by belly pain. Infants who have belly pain may pull their knees to their chests when they cry.
The pain of intussusception comes and goes, usually every 15 to 20 minutes at first. These painful episodes last longer and happen more often as time passes.
Other symptoms of intussusception include:
- Stool mixed with blood and mucus — sometimes referred to as currant jelly stool because of its appearance.
- Vomiting.
- A lump in the belly.
- Weakness or lack of energy.
- Diarrhea.
Not everyone has all the symptoms. Some babies have no obvious pain. Some children don't pass blood or have a lump in the belly. And some older children have pain but no other symptoms.
Adults
Intussusception is rare in adults. Also, because symptoms of the disorder often overlap with the symptoms of other disorders, it's more challenging to identify. The most common symptom is belly pain that comes and goes. Nausea and vomiting also may happen. People sometimes have symptoms for weeks before seeking medical help.
When to see a doctor
Intussusception needs emergency medical care. If you or your child develops the symptoms listed above, seek medical help right away.
In babies, pulling the knees to the chest and crying are often symptoms of belly pain.
Causes
The intestine is shaped like a long tube. In intussusception, one part of the intestine — usually the small intestine — slides inside a part next to it. This is sometimes called telescoping because it's similar to the way a collapsible telescope slides together.
In adults, the telescoping sometimes is caused by a growth in the intestine, such as a polyp or a tumor, called a lead point. The typical wavelike contractions of the intestine grab this lead point and pull it and the lining of the intestine into the bowel ahead of it. In most people, however, no cause can be found for intussusception.
Children
In most children with intussusception, the cause is unknown. Intussusception seems to happen more often in the fall and winter. And because many children with the condition also have flu-like symptoms, some experts suspect that a virus may play a role in the condition. Sometimes, a lead point can be identified as the cause of the condition. Most frequently, the lead point is a pouch in the lining of the small intestine, a condition called Meckel diverticulum.
Adults
In adults, intussusception is usually the result of a medical condition or procedure, including:
- A polyp or tumor.
- Scarlike tissue in the intestine, known as adhesions.
- Recent abdominal surgery.
- Swelling in the intestines due to diseases such as Crohn's disease.
Risk factors
Risk factors for intussusception include:
- Age. Children — especially young children — are much more likely to develop intussusception than are adults. It's the most common cause of bowel obstruction in children between the ages of 6 months and 3 years.
- Sex assigned at birth. Intussusception more often affects boys.
- Intestinal formation at birth that is not typical. Intestinal malrotation is a condition in which the intestine doesn't develop or rotate correctly. This increases the risk of intussusception.
- Other health conditions. Some conditions can increase the risk of intussusception, including:
- Cystic fibrosis.
- Henoch-Schonlein purpura, also known as IgA vasculitis.
- Crohn's disease.
- Celiac disease.
Complications
Intussusception can cut off the blood supply to the affected portion of the intestine. If left untreated, the lack of blood causes the tissue of the intestinal wall to die. Tissue death can lead to a tear in the intestinal wall, called a perforation. This can cause an infection of the lining of the abdominal cavity, known as peritonitis.
Peritonitis is a life-threatening condition that requires immediate medical care. Symptoms of peritonitis include:
- Belly pain.
- Swelling in the belly area.
- Fever.
- Vomiting.
Peritonitis may cause your child to go into shock. Symptoms of shock include:
- Cool, clammy skin that may be pale or gray.
- A weak and rapid pulse.
- Breathing that may be either slow and shallow or very rapid.
- Anxiety or agitation.
- Extreme listlessness.
A child who is in shock may be conscious or unconscious. If you suspect that your child is in shock, seek emergency medical care right away.
Diagnosis
A healthcare professional typically starts by getting a medical history and a timeline of when symptoms started. A sausage-shaped lump may be felt when the belly is pressed. To confirm the diagnosis, imaging tests may be done, including:
- Ultrasound or other abdominal imaging. An ultrasound, an X-ray or a CT scan may show an intestinal blockage caused by intussusception. Imaging results typically show a "bull's-eye" where the intestine is coiled within itself. Abdominal imaging also can show if the intestine has been torn, called perforation.
Treatment
Treatment of intussusception typically happens as a medical emergency. Emergency medical care is needed to avoid severe dehydration and shock, as well as prevent infection that can happen when part of the intestine dies due to lack of blood.
Treatment options for intussusception may include:
-
A water-soluble contrast or air enema. This is both a diagnostic procedure and a treatment. If an enema works, further treatment is usually not necessary. This treatment can fix intussusception 90% of the time in children, and no further treatment is needed. If the intestine is torn, an enema can't be used.
Intussusception happens again up to 10% of the time, and the treatment will usually have to be repeated. It is important to consult a surgeon even if treatment with an enema is planned. This is because of the small risk of a tear or rupture of the bowel with this therapy.
- Surgery. If the intestine is torn, if an enema does not correct the condition or if a lead point is the cause, surgery is needed. The surgeon frees the part of the intestine that is trapped, clears the blockage and, if needed, removes any of the intestinal tissue that has died. Surgery is the main treatment for adults and for people who are suddenly ill.
Sometimes, intussusception may be temporary and go away without treatment.
Preparing for your appointment
Emergency medical care is needed to treat intussusception. You may not have much time to prepare for an appointment.
What to expect from your doctor
Your child's healthcare team is likely to ask you several questions, including:
- When did your child begin experiencing stomach pain or other symptoms?
- Does your child's pain appear to happen all the time or does it happen off and on?
- Does the pain begin and end suddenly?
- Has your child experienced nausea, vomiting or diarrhea?
- Have you noticed any blood in your child's stool?
- Have you noticed any swelling or a lump in your child's belly?
What you can do in the meantime
Don't give your child any nonprescription medicines to treat symptoms before the appointment. Don't give your child anything to eat if you see any of the symptoms of intussusception. Seek medical help right away.
© 1998-2026 Mayo Foundation for Medical Education and Research(MFMER). All rights reserved. Terms of Use